Sunday Jul 05, 2026
Sunday Jul 05, 2026
Tuesday, 19 September 2017 00:00 - - {{hitsCtrl.values.hits}}

Data collected through the DHS deepens and transforms the understanding of population, health and nutrition issues in the country. As far as possible, the DHS uses consistent survey methods and questionnaires to measure key indicators, including infant and child mortality, fertility, family planning use, maternal health, child immunisation, malnutrition levels, HIV prevalence and more – Pic by Shehan Gunasekara
By Dr. Amara Satharasinghe
The Department of Census and Statistics (DCS) takes steps to identify, collect, analyse and communicate the information needed for the development programs of the country. For this purpose, the DCS and the Ministry of Health, Nutrition and Indigenous Medicine collaborates to update and expand the database on a number of crucial aspects of health.
The purpose is to provide information for evidence-informed decision making in enhancing the effectiveness of health service delivery. Health service delivery is guided by the health needs of the population. It involves assessing the health status of the people, analysing the causes, and incorporating the knowledge gained in refining programs and policies. 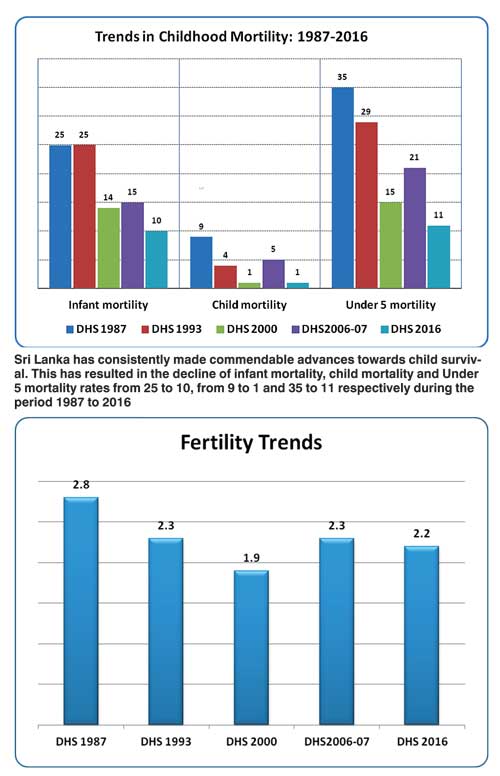
Current information is also essential for monitoring progress, proactively taking corrective action including strategic, legislative and policy enhancements, and advocating for desired levels of funding. To promote the essential process of evidence-informed decision making and action, the DCS in collaboration with the Ministry of Health, Nutrition and Indigenous Medicine conducted the Demographic and Health Survey (SLDHS) 2016.
Increasing emphasis by planners and policy makers on the utilisation of objective indicators for policy formulation, planning, and measuring progress has increased the reliance on regular household survey data, given the inadequate availability of appropriate information from administrative statistics and other routine data-collection systems. Demographic and Health Surveys (DHS) are conducted in many countries to provide quality data related to health sector for policy development and programme planning, monitoring and evaluation. The DHS collects a wealth of health related information on a wide range of topics, which are important for informed decision making in the health sector of the country.
DHS evolved from the World Fertility Surveys and the Contraceptive Prevalence Surveys implemented in the 1970s and 1980s. Like their predecessors, the DHS originally collected comparable population-based data on fertility, contraception, maternal and child health, and nutrition in developing countries. Today, the DHS core questionnaires are based on the best of scientific and technical knowledge and decades of survey experience. They are standardised and well-tested internationally and adapted for country contexts. In addition to the core topics, countries choose to collect data on special health issues including human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS), malaria, and domestic violence using optional modules.
The Department of Census and Statistics (DCS) conducted the fifth Sri Lanka Demographic and Health Survey (SLDHS) in 2016, which is the first ever DHS conducted countrywide, at the request of the Ministry of Health and Indigenous Medicine. The SLDHS 2016 is a follow-up to the 1987, 1993, 2000 and 2006/07 Sri Lanka Demographic and Health Surveys. This survey was funded by the World Bank under the Second Health Sector Development Project (SHSDP) – Component II. Data collection took place from May to November 2016. ICF provided technical assistance.
Survey objectives
The SLDHS 2016 was undertaken to address the needs of the health sector programmes. The survey was designed to provide policy makers in the Ministry of Health and other organisations with information for effectively planning, monitoring, and evaluating future interventions both at the national and regional levels, especially health sector activities. Specifically, the 2016 SLDHS collected information on maternal and child health, reproduction and fertility preferences, family planning, evaluation of maternal and child health services, women’s status, and knowledge and behaviour regarding HIV/AIDS and other sexually transmitted diseases, etc.
Sample design
A nationally representative sample of 26,178 housing units was selected for the survey and 27,210 households in these housing units were enumerated to provide district level estimates. Within the households interviewed, a total of 18,540 eligible women were identified, of whom 18,302 were successfully interviewed. Detailed information was collected from all ever-married women aged 15-49 years about themselves and their children born after January 2011. All women age 15-49 in selected households were eligible for individual interviews.
ICT tools for enumerations
For the first time, the Computer Assisted Personal Interview (CAPI) technique was used to collect data in this survey by the DCS. CAPI refers to interviews conducted using hand-held devices such as tablets or ultra-mobile personal computers. The questionnaire is configured using CAPI software and is loaded on to the device. The enumerator reads the questions to the respondent, and inputs the responses directly into the device. This electronic data capture approach eliminates the need for post-interview data entry and thus allows for immediate data retrieval leading to improved quality and timeliness of statistics. Previously, with pen-and-paper interviewing (PAPI), the responses had to be transferred to digital format through manual data entry after the interview. DCS now uses this technology for its surveys.
Key findings
Data collected through the DHS deepens and transforms the understanding of population, health and nutrition issues in the country. As far as possible, the DHS uses consistent survey methods and questionnaires to measure key indicators, including infant and child mortality, fertility, family planning use, maternal health, child immunisation, malnutrition levels, HIV prevalence and more. Therefore, data from these surveys are comparable across time and regions. Some of the key findings of the SLDHS – 2016 are given below.
Access to amenities
Ninety percent of the households have access to an improved source of drinking water with the majority of them having a water source on premises (80%, an increase from 72% in the 2006 SLDHS). Equally, importantly, 90% of the households and population have access to improved sanitary facilities.
As per household amenities/possessions, it was revealed that almost all households (97%) have access to electricity (increased from 80% in 2006). Two thirds, or 66% use wood and solid fuel for cooking (down from 79% in 2006) and TV and mobile phones access has substantially increased to 87% and 91% respectively (from 77% and 39% respectively in 2006).
Education
The 2016 SLDHS confirmed high levels of participation in education across the country with a median of 9.4 years (9.4 years for females and 9.2 years for males) of education. Primary school attendance is almost universal, while net school attendance in secondary education is as high as 83%.
Ever-Married
Women (E-MW)
The distribution of E-MW by place of residence, ethnicity, and religion confirmed previous distributions: 81% rural residence, 76% Sinhalese, and 71% Buddhist. Ninety percent of E-MW were currently married, 4% were living together and 6% were widowed, divorced or separated. Only 18% of E-MW had ever used internet and 16.4% used it during the last 12 month. One out of three E-MW reported as employed during the week before the survey. Age at first sexual intercourse of E-MW was 23.5 years, but 12% of them reported at age of 18 years. The median age at first marriage of E-MW was 23.7 years, but 12% of them had married exactly at the age of 18 years.
Fertility
Fertility has continued to decline to values approaching replacement levels including in all sectors. The 2016 SLDHS reports a TFR of 2.2 children per woman of reproductive age. Substantial changes were observed among adolescents and young people (15-19 and 20-24). The TFR levels, trends and observed changes are well supported by the observed values under the basic determinants of fertility, such as marriage and contraception. The median age at first birth has also increased substantially to 25.6 years. In addition, only 3% of teenagers reported a live birth or to be pregnant at the time of the survey.
Contraception
Contraception and contraceptive methods are universally known in Sri Lanka. Seventy two percent of the currently married women had a demand for contraception in 2016. Of these, close to two out of three (65%) currently married women were using contraception. The remaining 7% have an unmet need for contraception. Of the total demand for contraception, close to 90% of the demand for contraception is satisfied, mainly by modern contraception.
Increase in the level of contraceptive use was observed among adolescents and young adults 20-24, particularly in the use of IUDs and Implants. Although 35% of the currently married women were not using contraception, only 8% had an unmet need for contraception. The public-sector act as the main provider of contraception (97% for IUD, 99% for implants, 94% of sterilisations and, 57% for pills). The private sector’s participation is strong for the provision of injectable (68%), male condoms (61%) and pills (43%).
As for informed choice, there are still challenges. For example, only 53% of current users were informed about side effects. Further, only 50% were told what to do in case of experiencing side effects and only 42% were informed about other available methods.
Child mortality
Under-five mortality or deaths of children under five years of age computed from the SLDHS 2016 was 11 per 1,000 live births (from 21 in 2006). Infant and child mortality has continued to decline during the last 10 years.
Reproductive health
Ninety nine percent of the pregnancies in the country received antenatal care: assistance from health facilities (95% visiting health facilities during the first month of pregnancy, 96% attended by health personnel and, 80% protected against neonatal tetanus).
Almost all births had taken place in a health facility (94% in public and 5% in private). As for postnatal care, 99% of the births received assistance within two days of birth. Unfortunately, 16% of the births were low birth weight (less than 2500 grams at birth). In eight districts, this percentage was 18% or greater.
In terms of illness affecting children under the age of five 2.4% were affected by acute respiratory infections (ARI); 14.3% by fever, and 2.7% by diarrhoea (all below the levels observed in 2006). Almost all mothers (97%) knew about ORS; 91% of the mothers were aware about the proper ways of stool disposal.
Nutrition status of children and women
The prevalence stunting (height for age) among children under five years of age was 17% while prevalence of underweight (weight for age) and wasting (height for weight) were 21% and 15% respectively. Among ever-married women, 9% were found to be thin, 32% overweight, and 13% obese.
The majority (90%) of children were breastfed almost immediately after birth (98% within one day). Almost all households (95%) had supplies of iodised salt at home.
HIV/AIDS
Almost all ever-married women (93%) had heard about HIV/AIDS but only one out of three (33%) had comprehensive knowledge of AIDS (prevention and misconceptions). Yet alarmingly, this value was only 24% among young adults aged 15-24 years. Ten percent of the ever-married women had been tested for AIDS but only 74% of them received the results from the test.
Status of women
The majority of ever-married women (83%) had access to a bank account and 78% used a mobile phone. Only 35% were making decisions related to their health care, 20% on purchasing household amenities and/or 16% on when to visit friends or family.
Health indicators of SDGs
The 2030 Agenda for Sustainable Development Goals (SDG) is the world’s first comprehensive blueprint for sustainable development. Launched at the end of 2015, this Agenda frames health and well-being as both outcomes and foundations of social inclusion, poverty reduction and environmental protection. From a health perspective, development can be said to be “sustainable” when resources – natural and manufactured – are managed by and for all individuals in ways which support the health and well-being of present and future generations.
Associated with each Sustainable Development Goal is a series of targets and each target is measured by one or more indicators. Many of the targets in the areas of good health, zero hunger, no poverty, quality education, gender equality, clean water and sanitation, and reduced inequalities can be measured at least indirectly from DHS surveys.
SLDHS 2016 compiled data for SDG indicators: Prevalence of stunting; prevalence of underweight and wasting; proportion of births attended by skilled health personnel; proportion of women of reproductive age (aged 15-49 years) who have their need for family planning satisfied with modern methods; proportion of ever-partnered women and girls aged 15 years and older subjected to physical, sexual or psychological violence by a current or former intimate partner in the previous 12 months disaggregated by type of violence and by age; proportion of women and girls aged 15 years and older subjected to sexual violence by persons other than an intimate partner in the previous 12 months, proportion of women aged 20-24 years who were married or in a union before age 15 and before age 18 etc. These indicators compiled from SLDHS 2016 can be used as baseline data for assessing progress towards the Sustainable Development Goals.
Conclusion
The report ‘Sri Lanka Demographic and Health Survey – 2016’ containing key findings of the survey: SLDHS – 2016, was launched on 18 September and the first copy of the report was presented to the Minister of Health and Indigenous Medicine at a ceremony held in the Bandaranaike Memorial International Hall, Colombo. A soft copy of the report is published in the website of the DCS: www.statistics.gov.lk.
Health is regarded by the World Health Organization as a fundamental human right, and health promotion is defined as “the process of enabling people to increase control over their health and its determinants, and there by improve their health”. The findings of the survey may be used for health promotion in concert with other strategies including education, community development, policy, legislation and regulation for preventing communicable and non-communicable diseases and/or even for realigning current health policies to match with current and future needs.
The above report contains only a few of the key indicators derived from SLDHS 2016. To build the policy and programmatic evidence base, DHS data must be further analysed by researchers following standard protocols and rigorous methods. As seen in the data presented above, Sri Lanka has made very impressive progress in many of the measured areas. Progress may be inadequate in others. The multiple reasons for slow progress in hard to change areas must be understood through scientific analysis.
Evidence from research for decisions and actions must be made accessible in user-friendly packages for assimilation and utilisation by policy makers and program managers. Current policies and programs can then be realigned as necessary for addressing the obstacles while maintaining the great achievements made so far.
(The writer is Director General, Department of Census and Statistics.)


