Monday Jul 13, 2026
Monday Jul 13, 2026
Wednesday, 21 September 2016 00:01 - - {{hitsCtrl.values.hits}}

By Daniel R. Lucey
A UN High-Level Panel appointed 2 April 2015 by Secretary-General Ban Ki-moon stated in its 25 January 2016 report titled Protecting Humanity from Future Health Crises: Report of the High-level Panel on the Global Response to Health Crises that, “The Ebola outbreak in West Africa was a preventable tragedy. If the outbreak had been detected faster, and concerted international action had been mounted more rapidly, the spread of the disease could have been contained, and thousands of lives could have been saved.”
One contributing factor was the delay between the laboratory-confirmation of Ebola virus as the cause of the epidemic in March 2014 and when the World Health Organization (WHO) declared it a “Public Health Emergency of International Concern” (PHEIC) in August 2014. To apply this lesson learned from Ebola to the next potential PHEIC, in January 2016 an early call-for-action was published asking the WHO Director-General to convene “immediately” the Emergency Committee to advise whether a PHEIC existed due to the multination spread of Zika virus and the link to microcephaly reported in French Polynesia and Brazil by November 2015. (Lucey D, Gostin L. JAMA 2016 (Jan 27);315(9):865-66.)
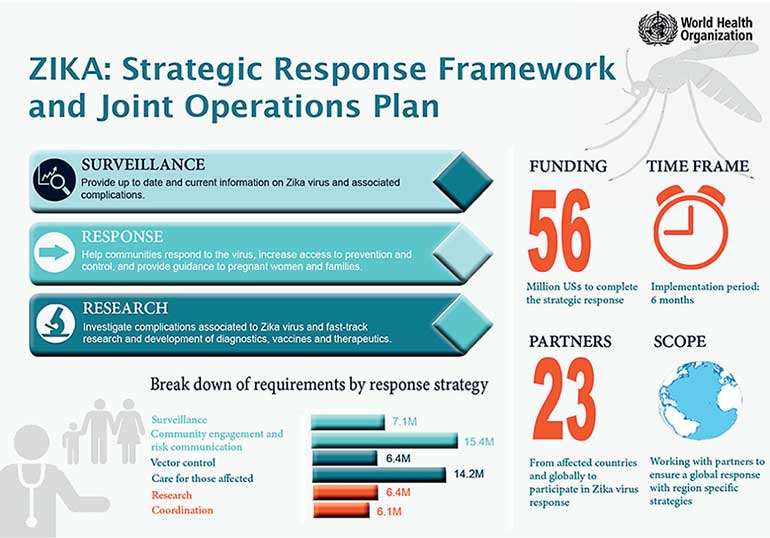
The WHO Director-General did convene this Committee on 1 February 2016, and declared a PHEIC focused on the clusters of microcephaly and neurological disorders, rather than the virus itself. Since then, under the leadership of the WHO in Geneva, international responses have been rapidly accelerated within a “Strategic Response Framework”, partly based on lessons learned from Ebola.
On 17 March a second early call-for-action was published (Lucey D. Health Security). This call was to offer assistance to the West African island nation of Cabo Verde in order to help identify children born with microcephaly following the Zika epidemic that began in early autumn 2015. By coincidence, WHO announced on 18 March that they were sending such a multidisciplinary team to assist Cabo Verde, at the request of their Ministry of Health, after a baby with microcephaly was born there on 14 March. On 31 March WHO reported another baby from Cabo Verde with microcephaly that was born on 24 March in the United States. Initial reports that day of Zika laboratory tests included neutralising antibody in the first baby and mother, and anti-Zika IgM in the serum of the mother of the 2nd baby. These babies with microcephaly linked to Zika infection are the first ever reported in Africa. There is anticipation of more cases being recognised in the coming months.
In this same 31 March report WHO noted Colombia, Panama, and Martinique, in addition to Cabo Verde and French Polynesia, have reported one or more cases of microcephaly with laboratory evidence of Zika infection. In addition, Brazil has reported 944 cases “confirmed with microcephaly and/or other neurological malformations suggestive of congenital infection” and over 4,200 suspected cases are still being evaluated.
The third early call-for-action, published in the same 17 March paper, requested diagnostic tests for Zika virus be made available in continental (West) Africa, including the three nations devastated by Ebola from 2013 to 2016. The goal was to recognise prospectively in Africa what was only recognised retrospectively in Latin America, when Zika virus likely traveled to Brazil from one or more Pacific islands. The opinion that African strains of Zika do not cause microcephaly, or that immunity against Zika is widespread across the entire continent, are not supported by data. As of 5 April, confirmation has not been reported as to whether the African or Asian strain of Zika virus is in Cabo Verde. Since at least 21 March the US Centers for Disease Control has been willing to help provide national reference laboratories in W. Africa with their new diagnostic test for Zika, Dengue, and Chikungunya, the Trioplex rRT-PCR Assay.
3 career lessons in 3 words: Anticipate, Recognise, Act
If a medical career beginning as a visiting US medical student at Baragwanath hospital in Soweto, South Africa in 1979 through 37 years in infectious disease clinical care, research, public health, and policy could be condensed into three lessons for going forward in 2016 they could be: (1) Anticipate (2) Recognise (3) Act.
These lessons are based on work involving infectious disease outbreaks in the United States from AIDS (1982 in San Francisco, to Boston, San Antonio, Bethesda, DC, and overseas) to anthrax (2001 in DC), and by traveling abroad to meet with medical and public health colleagues during SARS (2003) in China and Canada, H5N1 avian influenza in Thailand, Vietnam, Indonesia and Egypt (2004 to 2015), pandemic influenza in the USA and Egypt (2009), MERS in the Middle East (2013 to 14) and Korea (2015), Ebola in Sierra Leone and Liberia (2014 to 15), and Zika in Recife, Brazil (9 to 16 February 2016).
Anticipate
To a large extent, anticipating future events requires understanding past events i.e., “What is Past is Prologue”. In the example of the epidemics of Zika virus from the islands in the Pacific to continental Latin America, to islands in the Caribbean and islands in West Africa (what I would term “Pan-Epidemics” to avoid debates over the term “pandemic”) the pivotal event in making the first early call-for-action to WHO was learning in January 2016 that French Polynesia had reported (retrospectively on 24 November 2015) an increase in microcephaly and other abnormalities in 2014 to 2015 following their Zika epidemic in 2013 to 2014. Thus, the growing epidemic of “microcephaly and/or other neurological malformations suggestive of congenital infection” in Brazil in 2015 to 2016 had been preceded by similar but smaller events in French Polynesia.
Therefore, the international community should anticipate, and prospectively monitor for, pan-epidemics from the Pacific to Latin America and West Africa of microcephaly and Zika neurologic syndromes (what could be termed “ZNS”) both congenital and in adults (e.g., Guillan-Barre, meningoencephalitis, myelitis). Of note, the pan-epidemic waves of microcephaly and congenital neurological syndromes could be predicted not to start until approximately 6 to 8 months after the onset of a Zika epidemic, given the timeline of pregnancy and the (still-uncertain) proportion of pregnant women in whom Zika infection affects the fetus.
Recognise
In the example of the Zika pan-epidemics, microcephaly, and Zika Neurologic Syndromes (ZNS) the pivotal “recognition” event was cited above in terms of French Polynesia’s official report 24 November 2015. Even after an event is “recognised”, in terms of being “detected”, the importance of the event still must be recognised in order for appropriate action to be taken. Recognition of the importance of the link between Zika and microcephaly in both French Polynesia and Brazil required taking appropriate action, such as convening the WHO Emergency Committee (PHEIC), in anticipation of pan-epidemics of microcephaly and ZNS occurring in the many other nations and territories with Zika epidemics.
Some additional examples of when epidemics were occurring, but went undetected or unrecognised, are given below. Again, even when “recognised” in the sense of being detected, their importance still had to be “recognised” in order for appropriate action to be taken e.g., Zika in Brazil: December 2014 to May 2015; Ebola in Guinea: December 2013 to March 2014; MERS in Jordan: April 2012 in Zarqa November 2012 (retrospectively); H1N1 Influenza in Mexico: February 2009 to April 2009; SARS in China: November 2002 to March 2003; AIDS from prior to 1959 until 1981.
Act
There are no “lessons learned” except those proven by actions taken. At the risk of being wrong, sometimes action must be taken before all the desired information is available. Such early action can be essential when the consequences of not acting early enough can be catastrophic, as in the “preventable tragedy” of Ebola. With regard to Zika, microcephaly, and ZNS it remains to be seen whether history decides that the WHO Emergency Committee to consider declaring a PHEIC should have been convened sooner than 1 February, given the retrospective report from French Polynesia in November 2015 linking Zika and microcephaly. Even at the time the PHEIC was declared in February, only French Polynesia and Brazil had reported cases of microcephaly linked to Zika virus.
Looking at the WHO PHEIC declaration regarding Ebola in August 2014, and the PHEIC declaration regarding clusters of microcephaly and neurologic disorders possibly linked to Zika in February 2016, should there be a change made in 2016 from the current system whereby only one person, the WHO Director-General, has the authority to convene the WHO Emergency Committee to advise on whether or not an event should be declared a PHEIC? The next PHEIC might already be underway now in our world, albeit unrecognised.
Thank you for the invitation from UN Academic Impact to offer this commentary on how career lessons, including providing hands-on care for many patients with Ebola in West Africa in 2014, influenced the early calls-for-action against the rapidly growing pan-epidemic of Zika Neurologic Syndromes (ZNS) and microcephaly including in Cabo Verde, West Africa.
[Daniel R. Lucey is a Senior Scholar with the O’Neill Institute for National and Global Health Law. Dr. Lucey is an adjunct professor of microbiology and immunology at Georgetown University Medical Center (GUMC) and is a Senior Scholar at the O›Neill Institute. A physician trained in infectious diseases and public health, he has taught for 11 years at Georgetown on global emerging infectious diseases. He completed his infectious disease training and MPH at Harvard and worked in the US Public Health Service at the National Institutes of Health. His infectious disease training and MPH were at Harvard 1985-1988, after medical residency at UCSF, and medical school and college at Dartmouth. After working at the NIH and Washington Hospital Center until 2002, he co-founded a graduate program on emerging infectious diseases and biohazardous threat agents at GUMC. He has traveled widely in Asia, Africa, and the Middle East to exchange information regarding infectious diseases such as SARS, influenza, Nipah, HIV, anthrax, and MERS. Dr. Lucey is an author on over 100 papers and book chapters.]

