Sunday Jul 05, 2026
Sunday Jul 05, 2026
Tuesday, 18 May 2021 00:15 - - {{hitsCtrl.values.hits}}

Let’s focus on symptoms please. They don’t lie. Let’s treat the sick, let others get infected, and develop immunity naturally and via vaccination if need be. We have to get on. This is how every virus in history was tamed – Pic by Shehan Gunasekara
 Throughout the tapestry of confusions that has made up the pandemic saga we have been told to ‘follow the science’. Sadly, the recent steps taken by our Government show that, in the main, they are not being well-advised, and we are instead ‘fleeing from science,’ abandoning good management and communication norms, and even leaving the shelter of clear logic.
Throughout the tapestry of confusions that has made up the pandemic saga we have been told to ‘follow the science’. Sadly, the recent steps taken by our Government show that, in the main, they are not being well-advised, and we are instead ‘fleeing from science,’ abandoning good management and communication norms, and even leaving the shelter of clear logic.
Bizarre reporting and an outdated pandemic playbook
On 12 May late at night, the earlier tally of some 1,400 positive tests (posing as ‘cases’, not the same thing, ‘cases’ require symptoms before Covidian doublespeak took over), was added to and we were advised we now had ‘2,500’ cases. I always wonder at the daily 1-2 punch. A number is given by around 6 p.m. Then 700 or so ‘appear’ around 10 or 11 p.m. Where have they been hiding? On this date, if you read below the headline though, the number given is 2,386, consistently in each report, despite the 2,500 headline. Worldometers ‘split the difference’ and made it about 2,400.
Given alleged case numbers virtually everywhere else, still a blip.
No deaths listed. Worldometers again recorded zero. Then 13th morning, 18 appeared tagged for the last day. As I’ve reported before, under the headline we are usually told, these deaths, which are usually 50% a brew of comorbidities (including things like cancer and multiple organ failure) and 50% C-19 pneumonia, came from five to six days of being aggregated. So not sure why they are compiled as a ‘daily’ total? Except insofar as it sparks further unfortunate panic…
On 14 May, 29 deaths stated, but from 9 to 14 May clustered together into a day? 13 of them from evident comorbidities, 17 from C-19.
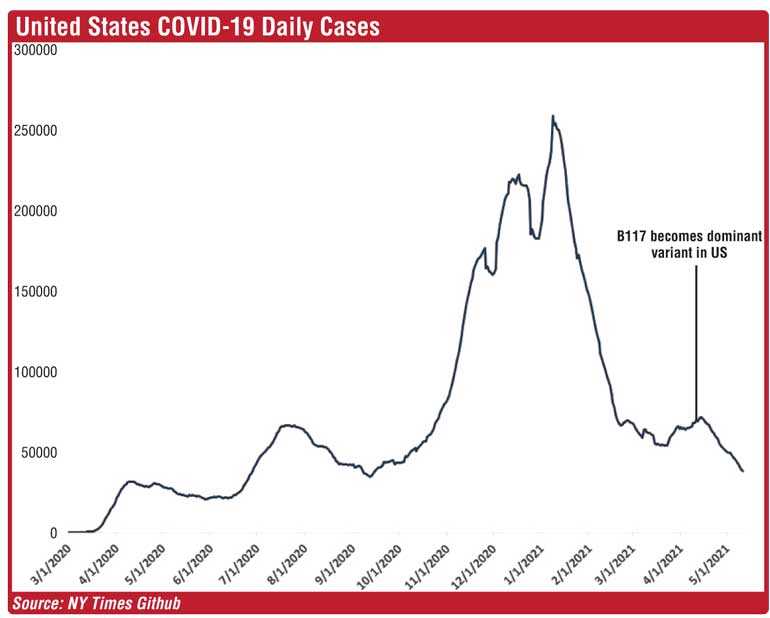
We have been told the UK variant is the dominant one in Sri Lanka. Weeks after that was confirmed as the dominant variant in the US, COVID numbers have been plummeting. The UK, where it hails from, is below a five-year average of deaths for 2021 despite the early year “surges.” So factually, giving it a brand name like “UK variant” or “B.1.1.7” doesn’t convey much of dire import given the factual track record where it actually had time to express itself.
Another bit of quasi-tabloid fear mongering has come from the IHME, University of Virginia, “modelling” which claims Sri Lanka may get 20,000 deaths. There is no point arguing over “models” at this stage. First, IHME has had a record of inaccuracies. The new regime overseeing them has well known political agendas. SAGE, whose models held the world captive, was forecasting 80,000 would die in Sweden since they had very lax restrictions, schools were open, face masks were optional. Sweden had an average “mortality” year despite a nursing home disaster (similar to the US and Italy) in 2020, and like the UK is below a five-year average to date for 2021. So much for “famous models”.
Biden advisor and infectious disease specialist Michael Osterholm who seems to rival Fauci and Ferguson for inaccuracy, forecasted publicly in January that the most “dire days” of the pandemic were upcoming, in the next 14 weeks after his proclamation. But then WHO finally admitted the PCR test is not by itself diagnostic and the Cycle Threshold (Ct setting) should be below 30. And so, well before any vaccine benefit could be asserted, the numbers began to decline precipitously. Amazing what a proper setting can do.
Over this period, more and more US States let go of masking, removed all restrictions, opened all businesses, many that had shut schools opened them. All of them had vast “declines” in C-19 cases and deaths, rather than vice-versa. So, a double whammy to the “expert” orthodoxy.
When about two months ago, Texas removed mask mandates and opened at large, Biden called them “Neanderthals,” experts were trotted out forecasting disaster and catastrophe galore. Deaths are actually down 75% since, case numbers have plummeted yet again, close to 58%. We were assured “death sentences” and “walking into the mouth of the beast”. While Maine, an orthodoxy posterchild, vastly masked and in parts locked down, has vertiginously climbing cases, Texas, when facts contradicted the paranoia, and the same in Florida and South Dakota and Mississippi and Georgia, not one acknowledgement from the media that earlier was frothing and doing death dances.
Hungary with avid mask mandates and movement restrictions, and as one of the most vaccinated nations on earth, has a far greater “death per million” ratio than India (which is quite mild on that basis compared to Europe or the US, less than one-fifth of those) and has huge spikes, while Sweden, with a few minor “case surges” is close to flat lining with no new cases on 12 May.
Why don’t we follow actual facts and data, and not fevered prognostications that are consistently wrong?
Why limit movement?
As I wrote in my last article, since we have been told by MIT, confirmed far and wide, that the virus is “airborne”, then I am fascinated by the logic of locking everyone up at home for three days over the long weekend and frankly even the travel restrictions.
We now know from the CDC studies that virtually no one gets infected from touching surfaces (one in ten thousand), and we are manically sanitising anyway. We are told, by no less than the NY Times a few days ago that there is not even “one recorded instance of outdoor transmission anywhere” when they took on the CDC claim that “fewer than 10%” of infections are outdoors.
That is true, but is akin to saying, “fewer than 20,000 people are bitten by sharks.” Also true, but the real number is 150 in the US. Ergo, that is both accurate and deceptive. Yes, it is fewer than 10%, fewer than 1%, as best we know zero, except ‘maybe’ in superspreader environments. Even there, the huge London protests of a few weeks back, throngs of unmasked people campaigning against lockdown, has led to further C-19 declines, and no surges in the two-week classic incubation period since.
So, our leaders are being terribly advised, to limit people leaving home. Even in the Lanka press we had clear reports that we need good ventilation, fresh air, sunshine. So, we opt to deprive the bulk of people of all of these, and the press reports say, government is limiting movement to stop the spread of the coronavirus. No, that may be the intention, but that is not what is being accomplished. What is being accomplished is trauma, stress, further business meltdown, imposition of hardship, for nothing.
If we don’t believe distancing and masks work, we should drop them. MIT says distancing is not really relevant, ventilation and crowding are bigger factors. “Locking up” an airborne virus makes no sense, and if you lock up those that are harbouring it, and then let them loose, it just circulates then. We’ve seen this play out in multiple post lockdown waves everywhere. It doesn’t work. Yet we keep insanely doing it.
It’s one thing to ban large events for a few weeks, but to inhibit people being outside, that is as close to “fleeing from the science” as it gets. And since the “positive tests” posing as cases are all over the Island, why is “travel” an issue anyway? Yes the “optics” look like “control” but it is disconnected causally from anything likely to make a difference. Again, Disney in Florida proves that every day, been open for many months, and Florida is 40th in terms of number of deaths now, despite one of the oldest populations and greatest urban density in the US, among the 50 US States. Science isn’t selective. It works or it doesn’t. Instead of bureaucrats with no track record in COVID success, why aren’t we consulting Taiwan, Vietnam, Sweden, Florida? None keep recurringly freezing their economies or their people.
A leading CEO told me the loss to their business in the upcoming 10 days from quarantine and travel restrictions will amount to $ 5 million! It would be fascinating if our advisers before proclaiming things that “flee the science” or are at the very least “highly uncertain”, would just ask actual businesses what the cumulative economic and commercial impact will be, and the human toll. Saying “human crisis versus economy” is complete bunk. The “human crisis” is speculative, given the death numbers, the economic toll is guaranteed, in an already besieged, teetering economy.
Hence the “lightest touch” possible is required by prudence. And the business I’m mentioning is just one overseas business, who will be explaining this shortfall to their head office, being part of a region, where they indicate to me, the others are relatively flourishing with far greater economic predictability and flexibility. “Survival” is a multi-faceted consideration, and not realising the “costs” imposed complying with continually changing requirements makes so many of our businesses potentially non-competitive.
When research says “don’t lock people in” why do we do the opposite, especially with such repercussions?
Surge questions
In early April we were testing about 7,000 people per day. By late April, about 14,000, by early May north of 20,000, with a number of days at 28,000 (at hopefully WHO and globally endorsed Ct settings), with 30,000 a day being the stated aspiration.
It doesn’t take a math whizz to figure out that the “surge” in “positive tests” (posing as cases) is partially explained by testing going up four-fold in this period. Even if “percentage” of positivity is up a few percent, 7,000 tests and 490 daily “cases” creates a very different degree of alarm than 30,000 tests and say 2,100 positive results.
So it is not the case that any of the variants have resulted in a mass quadrupling of cases, we are testing that many times as much, and even at the 5% sought for (set by who, or WHO, I don’t know, and on what basis never explained), 1,500 cases would show up, which would have been a “record” not long ago on any sustained basis.
So, we need to restrain our agitation over these optics.
 The question of treatment
The question of treatment
Peter McCullough is an Internist, Cardiologist and Professor of Medicine at Baylor, School of Medicine, one of the leading medical centres in the world. He has been involved in COVID treatment, and gives us the following bombshell:
Not only do most people recover from COVID, of those who do develop symptoms (of which a small percentage get hospitalised and die), they are “treatable” and close to 85% of even that small percentage then recover!
So, now we have paralysed a planet, and a country over a disease that is not only mildly lethal but also highly treatable!
Dr. McCullough with the doctors in Italy who were first on the European firing line in spring of 2020, published a paper in August 2020 in the America Journal of Medicine, arguing that we could intervene most effectively pre-hospitalisation and also vastly improve survival after hospitalisation.
He discovered to his shock that there were 50,000 peer reviewed articles on COVID, not a single one on how to treat it! When his paper was published, it became a lightning rod. He prepared a YouTube video, it went viral. And then was censored, leading to eventually to Senate testimony, and his recent testimony in Dallas.
With 57 authors he wrote a second paper, and so now there are exactly two papers on treatment! He points out that now anti-clonal antibodies are available, we are on even stronger ground. Has anyone ever read about these? Why not? Of all the COVID patients Dr. McCullough has treated since spring 2020, he has only lost two!
He says no one on the White House COVID task force has actually ever treated a COVID patient. That’s crazy! He indicates that any treatment has to treat three things: virus, the inflammation, and something to treat for the thrombosis. And very available, cheap and effective treatments like HCQ, Vitamin D, Zinc, Ivermectin, corticosteroids and now anti-clonal antibodies have demonstrably, globally made a difference. Why are they not at the forefront of public health discussions, and testing?
WHO has had a far from stellar record here. First, halting HCQ trials, then admitting the paper on which that was based was fraudulent, and restarting these trials, but far too late. Ivermectin they say they “don’t recommend” due to incomplete trials, which is ridiculous, it is widely used by WHO and the world for multiple decades, mostly as an antiparasitic drug. But it is a molecule in nature.
WHO’s own Dr. Andrew Hill having conducted months long, in-depth investigation, found a 74% reduction in fatalities associated with Ivermectin. Another WHO report states 81% but says it is not certain, and none of this even addresses its use preventively (WHO has no advice for preventive treatment!), as a prophylaxis, saying that falls outside their remit.
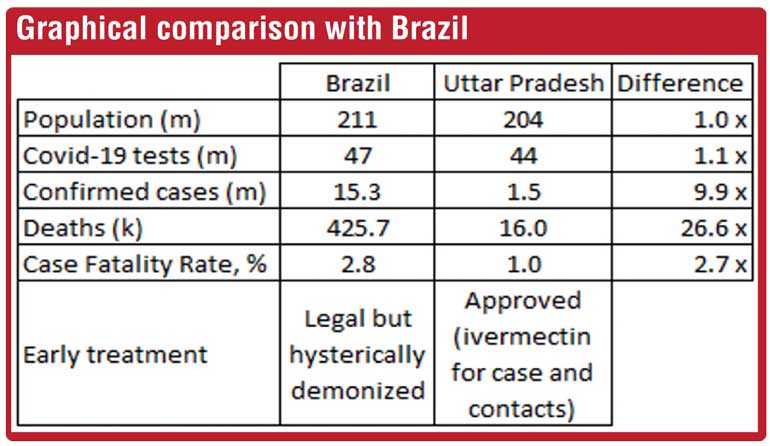
I urge all readers to read the most extensive and intensive coverage of this, peer reviewed by three of the most senior US scientists, with more than 15 randomized trials included, in the American Journal of Therapeutics, their currently highest ranked paper, https://journals.lww.com/americantherapeutics/Fulltext/2021/00000/Review_of_the_Emerging_Evidence_Demonstrating_the.4.aspx . Satoshi Omura who discovered Ivermectin, also fully supports its applicability re COVID. India is utilising it and links the downturn in key parts of India in part to its impact. The graphical comparison with Brazil is telling.
How not to communicate
We are told by the President, once more, “no island-wide shutdown” but provincial travel restrictions to be done in a way not to interfere with the daily lives of people.
Next day, we are told 11 p.m. to 4 a.m. essentially a “curfew”. Within a few hours we are then told, after having been assured yet again not to panic or buy up food or other essential supplies, that no, there would be “movement restriction”, the more pleasant name for “curfew” (or “like a curfew” as is curiously reported) for three days, over the long weekend! All this within a few hours!
We had already, on no science if keeping to 50% occupancy, killed all the hotel bookings through May that were keeping tourist sector afloat. Then, we had this weird injunction of being in a restaurant, but couldn’t drink there. Why not? Why further curtail profits, as the issue is only congestion, not what you are eating or drinking?
Then close swimming pools, despite fresh air, sunshine, exercise, zero outdoor transmissibility… more “fleeing from the science.” Ditto, parks and more, simply to satisfy the control fetish of various uninformed groups who get thrills from prescribing self-destructive shutdowns.
So we hear assertions, no strategy, no explanation, no one trusts anything. People are praying for a semblance of normal movement and commercial activity on Monday. We have proven none of us can control the virus. Maldives, along with Seychelles, among the most vaccinated places on earth, had the greatest current surges. So, we have to live with these spikes.
Can someone please explain, with no reference to “modelling” (which as explained have been catastrophically wrong throughout), on what basis 900 deaths justifies mass economic and social meltdown, losing businesses money, providing no predictability for anyone dealing with us, essentially scare mongering over a disease virtually everyone recovers from, and we now know is also treatable if we’ll bother to divert our energies there rather than shutting down the country?
Dr. McCullough also confirms, in all his treatment of COVID, no asymptomatic transmission, “sick people infect others”. My last article cited multiple studies also demonstrating this. So, we are holding our citizens hostage on what basis? Again, our leaders have navigated this fairly well to date, we mustn’t throw that all overboard.
And what’s the end game? Every few months, a new variant, PHIs take over again, GMOA campaigns for another weekend shutdown on no science, businesses can’t gear up for growth, as they need to perpetually “hedge” against quarantines, shutdowns, panic and psychological paralysis?
We want local tourism, but we don’t want anyone to travel? We want to keep hotels and restaurants viable, but people should avoid leaving home? We want profits for the exchequer, but we impose illogical restrictions. With no known game plan, we have a populace terrified, angry, jumping at viral shadows.
Let’s focus on symptoms please. They don’t lie. Let’s treat the sick, let others get infected, and develop immunity naturally and via vaccination if need be. We have to get on. This is how every virus in history was tamed. The infection fatality rate cited globally of 0.15% is not terrifying. Three million dead against global mortality over the same period of 80 million is not life altering. Almost 40% of even those came from care homes, and a large number from comorbidities.
Vaccines are for the vulnerable, most are on “emergency authorisation” only, not a solution. Only relevant for about 3-4%. South Africa with virtually no vaccination, has performed as well as massively-vaccinated Israel. Let’s look at data, not “talking points” and press releases.
Lead us please
For a disease 99% recover from, 85%+ of the rest can be treated for, with spikes in child hunger and 21% increase in maternal deaths from lockdowns in Lanka (the largest increase in South Asia), with deferred medical care, devastated education when children as per the science are not at risk (we just assert the new variants “may” affect the young, zero data to say so), imposing devastating business costs via quarantine panic and travel shutdowns…please, this pathogen doesn’t ooze out through pores.
We can keep playing this sad, painful “game”, but realise there is no endgame but the virus becoming endemic. We are shooting ourselves in the foot for nothing. I urge every reader to read the wisdom of so many eminent scientists: focused protection, apply readily available treatments, let those not at risk develop immunity. Stop publishing positive tests manically, and let’s get back to the desperately needed task of rebuilding this society and
economy.