Wednesday May 20, 2026
Wednesday May 20, 2026
Saturday, 9 October 2021 00:13 - - {{hitsCtrl.values.hits}}
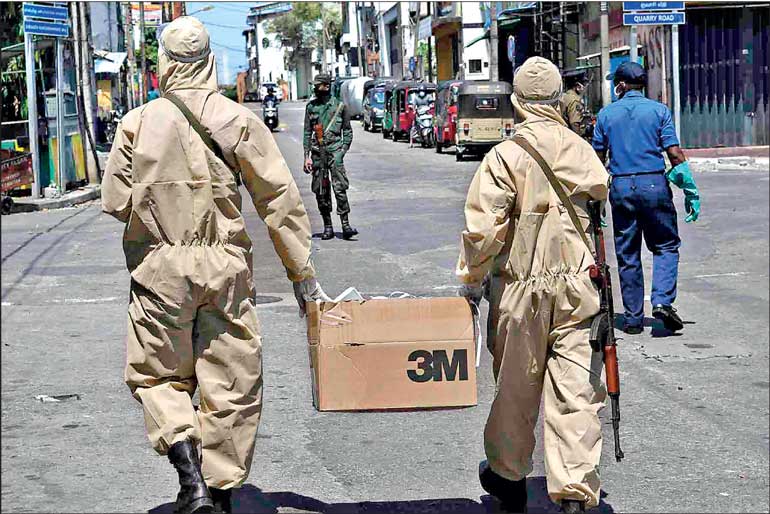
Nobody voted for human society to morph into an internment camp for a virus. It is time to reclaim our lives and liberties and use our stifled energies, to liberate them to enrich our communities and countries once more – Pic by Shehan Gunasekara
|
 A viral strain cannot be a peg by which we assess what we can and cannot achieve, who we can or cannot be, or the contours of social, economic and national destiny.
A viral strain cannot be a peg by which we assess what we can and cannot achieve, who we can or cannot be, or the contours of social, economic and national destiny.
Moreover, all the largely evidence free, almost madcap nostrums rolled out, have failed. Sweden, where they were ignored (no lockdowns, no mask mandates, no school closures) and sanity prevailed, boasts a lower all-cause mortality in 2021 than in 1991 (and many intervening years since). In the East Coast of the US, both infections and deaths are higher this “vaxxed” autumn than the preceding autumn. The same is true in the UK. Baffled we may be, but data is data.
Lockdowns, school closures, mask mandates have all flopped and backfired. Governments devastated their own societies with illogical, unsound, unscientific policies that we will be decades recovering from, and whose precedent will cast a shadow over civil liberties for quite some time to come.
The precautionary principle, the demand that cost/benefit assessments be done for major exceptional undertakings, is ignored to this day. If you visit www.rationalground.com, there is a chilling drop down menu of global collateral damage from the insanity of shutting down society to confront a virus with a 99% global recovery rate.
The costs have been staggering, ranging from tragic declines in mental and emotional health, suicide and addiction surges, crushing economic impact, the incalculable loss of education at critical developmental junctures, escalating health care costs, delayed and cancelled care for true killer diseases for hundreds of thousands (potentially millions) of patients.
Lockdown mania
And the concept “lockdown” is a brute instrument, as they are not all created equal. The Oxford Stringency Index looks at 9 measures on a scale of 0-100. The higher the number, the greater the restrictions. The Index found an inverse relationship between degree of stringency and positive public health outcomes.
Denmark having dropped all COVID restrictions (joined by Sweden and Norway), still hovers around 27 or so on the scale. Bangladesh is around 50 (essentially open and focusing testing on the symptomatic). Lanka had the most stringent rating of 86 (thanks to our curfew fetish…which happily is not really enforced of late), until Palestine overtook us. So, the degree of restrictions, their nature, how targeted they are, their duration, all matter crucially.
Instead of protecting the vulnerable, the morbidity and mortality burden shifted to the underprivileged. After all, the underprivileged were kept from earning their wages. And there were swathes of people not “locked in” but delivering food and other distractions to the privileged, for whom it was a nice, extended, paid holiday. At least until the full extent of the economic impact comes home to roost.
As virtually all spread is indoors, and the pathogen was airborne, we created the absolute worst environment we could for transmission. And beyond that, according to the US CDC, the two biggest comorbidities are obesity and anxiety. So, we fostered the first by locking people in, and stoked the second incessantly through 24/7 panic porn!
It is perverse. If truly at risk, what we did was tantamount to dispassionately asking those who have to work, to expose themselves to supply the “necessities” (lattes included of course) to the affluent, while sacrificing their own health and safety. Of course, the virus in terms of lethality below 65 for the healthy is a dud, so the privileged kept pointlessly cowering, walking the dog, tending to their garden, pontificating at leisure, awaiting vaccines as salvation (without bothering to learn that these “vaccines” as per their own EUA never were aiming at sterilising immunity). SMEs were devastated, daily wage earners repeatedly facing poverty.
In many countries, the elderly were confined to nursing homes, which extended the window of exposure to them, repeatedly exposed to staff who potentially brought infection into those cramped settings where, without attention paid to ventilation, infection potentially spread like spitfire. Lower risk people, far from also being locked in, should have been living naturally and contributing towards population immunity. Not having movement, with mobility constrained, as Australia and New Zealand are now learning, only delays the inevitable.
As we have repeatedly pointed out, locking up the healthy is without precedent in history. Study after study, looking at actual data rather than models, confirms no positive impact from doing so. Florida, open for more than a year, despite a very elderly population and a positive test-based summer Delta surge, has better public health outcomes than perpetually masked, locked down California. And this is not surprising. Once we learned in the spring of 2020 through seroprevalence and other case studies, the actual age stratified, mildly lethal nature of COVID, the only rational thing would have been to focus on those at high risk rather than an unsustainable, unscientific and counterproductive, en masse freezing of life as we know it.
The unparalleled stupidity is further demonstrated when we note that the median age of death consistently, from February 2020 to August 2021 is between 82 to 83 years of age. In most nations this is at or actually slightly beyond life expectancy. Ergo, even with the almost criminal neglect of clearly efficacious, highly available and extremely affordable early treatments, mass panic was hardly warranted. And even if you were elderly and at high risk, you still had a 95% chance of recovery. Lives have not been shortened in general by this overblown ‘scamdemic’ and that we so mindlessly over-reacted to this without consulting and learning from developing data is something we shall ponder to our everlasting chagrin.
So, in short, we unravelled our societies for a virus with an infection fatality rate similar to seasonal influenza. Stanford professor John Ioannidis looked at 36 studies (with 43 estimates) plus an additional seven preliminary national estimates (50 pieces of data) and concluded that, below 70 years of age across the world, the IFR ranged from 0.00% to 0.57% with a median of 0.05% globally. So, the rate of survival for those under 70 is approximately 99.5% and the IFR is near zero for children and young adults. While anyone can be infected, there is therefore more than a 1,000-fold difference in the risk of death between the old and the young.
Here’s how to escape
The first step is to permanently ban a one-size-fits-all lockdown approach which is the equivalent of shooting ourselves in both feet: we destroy society without gaining any real immunity. We have to focus on those at risk and, for God’s sake, let’s stop tormenting our children. We should provide for those at-risk, effective prophylaxis and early treatment for those who are symptomatic – both are widely available.
An extremely effective prophylaxis regimen advocated by Dr. Shankara Chetty, who has pioneered a remarkable protocol that addresses recovery at the eighth day when the disease enters its inflammatory phase and has treated over 7,000 patients without one being hospitalised or dying is: Vitamin C and D, Zinc and Doxycycline 100 mg daily, and Ivermectin 12 mg/50 kg weekly.
We must allow physicians to exercise their best clinical judgement as to how to best treat their patients and remove any threats of discipline and punitive action for not following ‘the politics’ on matters of natural immunity or vaccine safety. In too many countries the sacrosanct nature of the doctor patient relationship has been sullied. This has led to the therapeutic nihilism of simply not treating patients, perhaps for the first time in medical history, until they need emergency care and are near death. Having begun with outpatient early treatment here (hurrah!), we must continue to study and apply clearly effective (based on global patient results) early sequenced multi drug treatment (combinations of anti virals, cortico-steroids, antihistamines and anti-thrombotic, anticlotting drugs).
Combined with the above, we need an understanding of the salvific role of vitamin D supplements, Zinc, exercise, well-ventilated spaces and more. These all have to be threaded together in our public health consciousness. And we need to communicate unequivocally that we cannot rationally act as if we are at equal risk of severe outcomes or death even if infected. The 85-year-old grandma with two to three medical conditions requires the best of our expertise and care, whereas a 16-year-old in the pink of health will readily recover and can be symptomatically treated as necessary without any undue panic.
We must also permanently ban spurious mass testing of asymptomatic persons particularly when the demonstrably flawed PCR tests never were authorised for mass testing of asymptomatics – in addition to all their other issues regarding cycle threshold (Ct) settings and false positives. And there should be no isolation of asymptomatic people. Where any temporary isolation is undertaken, there should be a very low Ct setting of the PCR test, below 28, and strong clinical suspicion that is corroborated.
Let’s dispense with the silly mask mandates unless in highly congested settings where we are worried about macro particles as opposed to the viral nano particles which the masks can do nothing for, any more than they could for cigarette smoke.
No lockdowns, business closures, school closures, as the crushing harms and degradation of life prospects far outweigh any nominal benefit. Harms are most pronounced among children whose lives and development are being compromised, perhaps irreparably, and the poorer in society who can least afford the restrictions. People are being killed through suicide, addiction or deferred care. Domestic abuse including child abuse skyrockets, job losses spike stress levels which are a major killer across the board and more. Once more, for our children in particular, when there is near zero risk from COVID, how dare we essentially destroy their lives over it?
Let us just admit that most of the ‘decisions’ made by governments and their medical advisors over this period were specious, reckless and harmful. Corrupt media ran interference for illogical actions like penal lockdown posing as medical advice. An almost unbearable toll fell on the public due to inept, badly executed and near dictatorial actions based on discredited models and which, on the data, are now proven to have no scientific basis. Open/shut repeated vacillation, based on a “positive test-demic” based on positive tests with unknown settings, potential lab contamination, and rife with false positives will never allow societies to regain confidence or momentum for recovery.
The vast majority of society, the ‘well’ and those with no underlying illnesses can take reasonable common-sense precautions and live normally. They will then, supported by early treatment if needed, naturally and by and large harmlessly, build a wall of natural immunity that protects everyone and facilitates the virus becoming endemic.
The vaccines as designed, do not protect an individual by the provision of ‘sterilising immunity.’ “Sterilising immunity” means that there would be neutralising antibodies and no further prospect of either getting infected by SARS-CoV-2 after being vaccinated or transmitting it on to others. Evidence from the Delta variant in particular shows palpable failure on both these fronts. Nor did the ‘vaccines’ in their EUA even purport to do other than protect against extreme symptoms and reduce the likelihood of death. Overall, a recent seminal and transformational Israeli study by Gazit et al. confirms that natural immunity clearly confers longer lasting and stronger protection against infection, symptomatic disease and even hospitalisation. UK data testifies to the same.
Proper safety surveillance systems are long overdue for these gene therapy ‘vaccines’ with a catastrophic number of adverse effects detailed on government data bases, despite every attempt to attribute these to coincidence when ‘reviewed.’ Brian Tyson MD points out that when you type ‘COVID-19 vaccine,’ and click on adverse reactions on the WHO site, vigiaccess.org, the stupefying number you get is 2.2 million!
And we have the temerity to even question the Nobel Prize winning drug (for its human application) Ivermectin with just under 4 billion doses and a little over a mere 4,000 adverse effects since 1992 (Aspirin has 177,606 since 1968, Remdesivir the prescribed COVID treatment which manifestly doesn’t work has 5,733 since 2020 alone, the C-19 vaccines had as of early 2021 a shocking 309,403 since 2020, now have swelled into the millions)? In terms of “deaths” the “vaccines” are over 30,000 by conservative count (US VAERS, EU and UK), Ivermectin has had 16 deaths attributed to it since 1992! So, said surveillance systems would feed into a real committee which would ensure this is conveyed so we have proper ethical and fully informed consent by the vaccinee as per the Nuremburg standards.
|
More ways to escape
There is virtually no asymptomatic spread. “Asymptomatic” unless someone’s immune system is naturally processing the infection, means “healthy.” There are no reliably documented cases of asymptomatic spread, certainly not with enough viral load to infect someone else. From JAMA meta-analysis to a 3-million-person strong Wuhan study, clinicians continue to say they have not encountered any reliable instance. WHO discourages mass testing of the symptom free now as well. Certainly, a PCR test will not suffice, until Ct setting is around 24 and there are symptoms consistent with C-19.
And yet again, a “case” is someone with symptoms, not someone who tests positive. So “case reporting” has to stop, flashing of “infection numbers” which if they don’t translate into symptoms are completely irrelevant. The mismatch in the UK continues to be striking, 35,000 daily “positive tests” and around 150 daily deaths ascribed to COVID.
We should not be vaccinating those not at risk, nor those who were infected and have recovered. Continual booster shots, with the equivalent of last year’s flu shot (as the variants have moved on, and to date the “vaccines” have not) is worrying, as we have no idea what injecting that amount of spike protein (which is what causes the COVID illness) into the bloodstream will lead to or produce.
Surely, we must also be disgusted by the blatant disregard for our children’s wellbeing inherent in C-19 policies. It is asserted that it is important to ‘immunise’ children ‘to maintain their education.’ Are we now living in a society where a child’s right to education is dependent on their participation in medical experimentation? Why are schools closed when evidence from numerous locations show there is no need to close them to protect those who are not at risk? Is it right to support this abuse of children’s rights as recognised under the United Nation’s Convention of the Child?
Studies from around the world have shown that a child’s risk of death from COVID-19 is miniscule, including a study from England showing that 25 children died with COVID-19 between March 2020 and February 2021. This was in a population of over 12 million children, with millions of cases of COVID-19. Most of these children also had underlying health issues. The US CDC cites no childhood mortality for any child without serious comorbidities.
Is it ethical to deny children and young people a robust and durable natural immunity to SARS-CoV-2, therefore? Is it ethical to subject them to the unknown risks of novel vaccine technology and potentially a lifetime of COVID injections?
And we must surely toss the masks for children in particular. They have no benefit whatsoever for them and negatively impact their development, emotionally, socially, health-wise in terms of oxygen flow and potentially the pathogens and bacteria the masks amass. We need to let children run amok again, get fresh air, interact with natural environments, let their natural mucosal immunity get taxed and tuned up daily as it was designed to. We are cueing up a disaster via locking them down and in, shutting down schools, outlawing social interaction. Human history testifies to our immune system’s genius, and the global recovery rates are crystal clear, especially in that age demographic.
And we must further ask, on what basis, did country after country discard years of pandemic planning when faced with SARS-CoV-2 in 2020? We must restore data and evidence tested policies and ideas and established public health and medical wisdom and not allow them to be discarded and replaced with coercive and incoherent lockdowns, border closures, forced PCR testing, digital surveillance, mandatory quarantine and what may be tantamount to coercive measures to impose this manic pharma profit drive masquerading as “the science”.
All this might be an “experiment” to modellers and public health prognosticators, but to millions and billions of citizens around the world – this tragic fiction has become fact. These asserted policies are a harsh reality that have resulted in the widespread suspension of civil and political rights and enabled the biggest power shift, in the relationship between government and citizens, in living memory. These policies are destroying the lives and livelihoods of everyday people – with those already experiencing socioeconomic hardship suffering the most of all. But the other casualty, is the progressive nature of human society. This is a disgrace.
And so…
We need courage not pointless fear. We cannot cower under our beds and await some “authority” to announce what our lives should be. Mass media hysteria and fear mongering about variants and mutations is best ignored, as if we let them play out, and society is open, ever milder variants are what get perpetuated (due to the survival instincts of the virus itself). The task forces and medical spokespeople have been persistently, consistently wrong. If really serving the public, why are a diversity of eminent voices not invited and consulted, instead of deplatformed and shamelessly censored?
With Sweden and Florida, and “lockdown light” Japan doing much better than those following the playbook, and keeping societies open besides, we have to look at what is viable, sustainable as well as sane based on evidence.
Nobody voted for human society to morph into an internment camp for a virus. It is time to reclaim our lives and liberties and use our stifled energies – to liberate them to enrich our communities and countries
once more.



 Lockdowns, school closures, mask mandates have all flopped and backfired. Governments devastated their own societies with illogical, unsound, unscientific policies that we will be decades recovering from, and whose precedent will cast a shadow over civil liberties for quite some time to come
Lockdowns, school closures, mask mandates have all flopped and backfired. Governments devastated their own societies with illogical, unsound, unscientific policies that we will be decades recovering from, and whose precedent will cast a shadow over civil liberties for quite some time to come