Sunday Jul 05, 2026
Sunday Jul 05, 2026
Thursday, 14 May 2020 00:00 - - {{hitsCtrl.values.hits}}
So, we are now in the midst of the “curfew that wasn’t” and the “resumption of normalcy” that “still isn’t.” We are teetering, curiously and perhaps pointlessly.
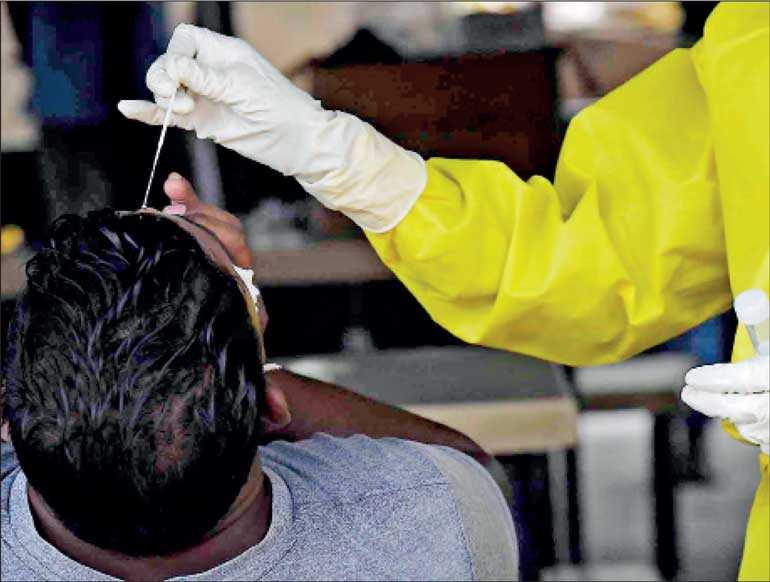
There was a report, which seems to track reality, that our encounter with COVID-19 in Sri Lanka has been a “tale of seven clusters.” If we leave out the Chinese lady who came afflicted, and went off cured, without seemingly infecting anyone, we have: Cluster of the Tourist Guide (11 March); Cluster of the Gem Merchant; Foreign Cluster (returnees from Italy; Dubai; etc.); Cluster of a group that returned from a religious event; Suduwella Cluster; Cluster from the “superspreader” family returning from India in Bandaranayake Mawatha; and the still spiralling Navy Cluster. The moment you state it as such, it affirms the medical position that we did not transition (fortunately) to wide-scale community transmission. In fact, quite a bit more than 500 of our cases come from the last two Clusters.
How we are still calling Colombo “high-risk” shows a complete immunity to facts. Just to bore you with a recitation of a few so called “high-density” cities in Asia: Tokyo (155 deaths among 12 million roughly) Hong Kong (4 deaths among 8 million), Taipei (6 deaths in all of Taiwan, 2.65 million in Taipei), Ho Chi Minh City (0 deaths among 9 million), and as previously indicated very small percentages against population in terms of mortality in Mumbai and Karachi as well.
And yet the “opportunity cost” to the economy of not letting Colombo really resume normal activity and life is more than 40% of GDP, even though with masks and prudent distancing and hygiene practices, there would be minimal chance of infection, and if it occurred, focused quarantining and isolation would be the rational way to address it.
For perspective
And we, here in Sri Lanka, in what was touted as a “bold” move, we ‘finally’, also on 11 May, let people go grocery shopping, which everyone else globally could do throughout (replete with photographs of military carrying weapons while heralding “resumption of civilian life” with the irony clearly lost on the photographers who have an evident martial fetish)!
We also had people return to their offices, though any business that needed customers needn’t have bothered, as people were only to leave home for “essentials.” So, either we render what is “essential” rather elastic (unavoidable if you need a haircut after 52+ days) or ask people to “stand guard” at their place of business, without being able to conduct any.
Tourist hotels were told by Police directive they could open, but not their restaurants! Since borders are closed, and no one is traveling into Colombo due to “curfew,” with no restaurants, bars, health clubs, operating at hotels, what is anyone supposed to “do” at these “open” hotels – a round of lawn tennis?
No, not allowed yet either!
As I wrote, if you can open a salon (yes please!), you can open a restaurant or a hotel lounge/bar, which is far more spacious, as long as you have occupancy/distancing guidelines. And let us let consumers give these poor folks some revenue, collect some for the State (which of course desperately needs it) and let’s stop shooting ourselves in the foot.
During the 38 seconds that the stock market was open on 11 May, among the hardest hit stocks were the hotel sector, not shockingly. Lanka Distilleries, an admired and celebrated company, has pointed out that their sector in Sri Lanka will face an impact of billions, having missed out on the holiday sales, an annual bellwether of demand for them. These are leading industries, and we keep insisting on banning bars (even those where physical distancing and occupancy guidelines can be practiced).
The entire industry provides crucially needed tax revenue, and so hearteningly, we have had a fascinating development on 13 May, with liquor sales at least allowed in non-curfew areas and via supermarkets in Colombo and Gampaha. The English translation uses the word “bar”, when it seems to clearly mean “store” at times, and so I cannot fully decode the liberties granted outside our perpetually curfewed zones. But we can applaud the forward movement, however infuriatingly incremental it may be. Hopefully, we will not again “panic” when pent-up demand is expressed. It is inevitable in the short run to some extent, and will peter out. Not an argument for depriving the exchequer of crucial liquidity, as the transition has to happen at some point.
Oh, we will likely hear the well intentioned wails: alcohol impairs immune systems. Yes, granted. But then so does driving in traffic to get to work, starving as daily wage earners with no income for months, losing your job, losing your business, having the financial system compromised, deferring needed medical treatment, being locked inside for two months while congratulatory headlines of “arresting curfew violators” keep flashing, not having children in school, losing your savings and more. So, surely it can’t just be “alcohol,” a legal product, which leading companies offer here, that we have to fear?
Publish the “circuit breakers,” keep policymakers making policies not surrogates, and let’s stop advocating for policies we cannot practically afford. How much do we have to lose to let this sink in?
10 reasons to end the “quasi-curfew”
Bonus question: do we need a tourism industry? If so, no overnight curfews, let hotel restaurants and bars operate, otherwise you cannot let them even start to get up off the proverbial mat where they have been “pinned” for months. This requires only basic economic horse sense to stipulate, affirm and confirm.
John Lee, former professor of pathology and NHS Specialist in the UK, penned this framework relative to the UK; I have adapted these insights for Sri Lanka. They apply in both cases.
Stop looking at case numbers. Mortality rates are what matter. And even in the US and UK, a growing percentage of the death tolls are now from nursing homes. Also, as so many are asymptomatic (we were told 50% of those infected in Lanka may be so by the Health Ministry), it’s a waste of time. The death rate is so miniscule compared to other causes of mortality, that this is becoming silly, despite this being a new, nasty, and (for some) dangerous virus. 94-99% of those who get the disease recover, 99.9% if you factor in the asymptomatic, and 90% of those who tragically are lost have pre-existing conditions. So, given that, the reason to finish off what’s left of the economy, rather than to let everyone get behind an economic rally, recover and move towards fresh resilience is…?
The initial response was due to “spikes” in certain countries who waited too long, and modelling which has been shown to be wildly erroneous, far too alarmist. All these models were biased towards severe cases.
Countries with very differing degrees of “lockdown” (virtually nowhere globally was there a close to two months’ “curfew” and a virtual closing of the entire economy) are having wildly different results. There is data from Israel, Sweden, and Hong Kong that suggests that the curve flattens around 50-70 days regardless, as long as there is some prudence re: mask wearing, distancing, hygiene, and isolation when there are symptoms. All this taken together suggests we may just be going through a shamanic ritual rather than medical necessity.
There is huge disruption to other healthcare due to our “curfewed lockdown.” But there is also the economic impact on health which is measured often by “quality of life years” or QALYs. So, a suicide, several years in poverty, educational loss that forecloses future choices or more, all “matter,” not just biologic survival, much as we wish to safeguard that as much as we can.
We cannot sustain this. Vaccines may never be found for an illness with this little mortality; the “immune response” we are told by experts cannot be predicted anyway. Different strains may emerge, and if we suppress our immune response, we may well pay for it “post-curfew”, or next season, or with the next viral pathogen. No country in the world has improved its health by making itself poorer either.
Since even most of the elderly recover, we are keeping them from the very things they bothered to stay alive for! Time with their families, hobbies, venturing out to favourite places, charity work, traveling. And we are finding now from global statistics, that more people were infected “locked in” (New York verifies this too), than those whose work had them out and about and moving around (we need real oxygen and sunshine to combat viruses, as we’ve known for centuries). As John Lee asks, using UK data, 10.8 million above 65 in England and Wales. Say, deaths there spike to 50,000. That’s still a 1 in 200 chance of death > 65. Might we ask people if they want to be locked up “for their own good” by the Government, or be allowed to live their lives as they wish and see their families and lifelong friends?
Everyone else, largely at modest to no risk, is having their lives decimated for no reason! Why is removing them from profitable activity, which could safeguard everyone, the solution? Because they might get infected and bring it back home? Not if prudent guidelines are maintained at work and at large as proven by Taiwan, Hong Kong, Vietnam, and outside of the foreign dorms by Singapore.
Why and how can we prioritise one disease over every other? Developing countries have postponed vaccinations for illnesses we actually have cures for, and we may next face waves of quite avoidable deaths on that basis. Cancer screenings and heart patient visits have been deferred. There are more of these than we can catalogue being “stockpiled,” though they will probably never make the front page of a newspaper.
While it is not settled science, it is an emerging medical view that asymptomatic people are not as contagious as those with symptoms, and when they spread it, a more mild and less virulent form is likely to be distributed, which as Dr. Lee argues is the evolutionary view of viruses, and what we want to have happen.
When it’s a matter of your life and livelihood, people will learn to behave sensibly, no matter what bias we may have about the aptitude of our own citizenry. Social responsibility in the face of a new and highly infectious respiratory illness is far more feasible and sustainable when it’s viscerally clear that eroding the economy and undermining the society you are sponsored by and literally depend on, is the alternative.
Let’s turn the page … please
Clearly, the world is shifting into a new phase, and we cannot be lagging behind.
I had always thought with our very limited caseload here in Serendib and extremely low fatalities, like Taiwan, we could have continued to offer services while other economies were closed, utilising focused isolation and quarantining. While that is now behind us, at the very least, we cannot be flagging now, while others increasingly step forth.
And there is much that is still being debated as to how extreme social distancing needs to be. Sweden has still embarked on relatively mild social distancing, though more voluntarily, with a largely open economy. While they have had many deaths (roughly half from nursing homes), it is a lower percentage than the UK, France, Netherlands, Belgium, Italy, Spain. Belarus, with almost the same population, and also no limit to gathering size (which Sweden has), but also keeping shops, restaurants, bars open, has only had 120 deaths in total. So, much still to be learned clearly. Yes, we can speak of despotism re Belarus, but that hasn’t seemed to help Russia.
That though does mean that while staying prudent and perhaps wishing to more take a medical leaf from Hong Kong and Taiwan and Ho Chi Minh City (which never really “locked down” their economies), or even New Zealand and Australia (which use the tiered “circuit breaker” model, and never went to curfew either), we should still pay attention too to these outliers.
Certainly, it merits challenging the lazy assumption that “extreme responses” that undermine economy and liberty are responsible for bringing this under control. And in Sri Lanka, it frankly was never “out of control” here, so we had nothing to rein in or “flatten.” We have more cases now than before, again though strictly due to identified clusters.
As the world re-opens, shall we re-join them, and not in this haphazard, on again/off again manner? We have to stop fretting over caseloads, as even of those small number “infected,” only a small minority of those will ever need intensive care. Let’s trust our excellent doctors and parlay the relatively “charmed” South Asian immunological profile that has people baffled insofar as mortality statistics go re India, Pakistan, Bhutan, Cambodia and more.
Our measures, now and going forward, as we commit to economic resilience and revival, have to be proportionate and effective, hopefully no more reflexive curfewing and indefinite undermining of key economic sectors. Hopefully, we can now commit to strategies that are not a “whisker” more ruinous, oppressive, or just out of step with global learnings, insights and best practice, than they absolutely need to be.


