Thursday Jun 04, 2026
Thursday Jun 04, 2026
Saturday, 5 December 2020 00:02 - - {{hitsCtrl.values.hits}}
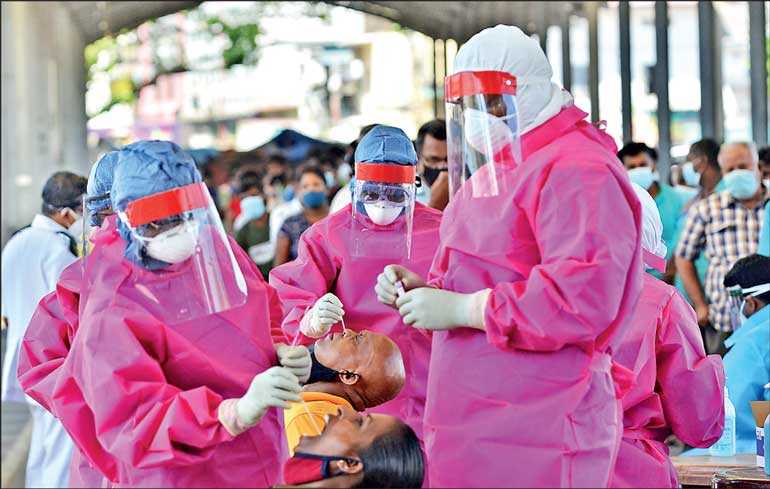
We should stop mass testing asymptomatic individuals. If still in doubt, five days of home quarantine, just in case. But since we are not in an epidemic in Sri Lanka by any definition of exponential growth of real ‘cases’ or ‘clear deaths’, mass testing has to be carefully justified – Pic by Shehan Gunasekara
 It seems every time we move forward, there is an outbreak of paranoia from some of the health unions and some elected officials telling us to remember to continue to quake in our proverbial boots. ‘Global pandemic,’ ‘PCR tests’ and whatnot. Hearteningly, the policymakers and Government leaders have been taking a sober, balanced cost/benefit approach, increasingly focusing on a twin inescapable set of priorities: ‘Lives AND Livelihoods.’ One without the other is a chimera, a pure illusion.
It seems every time we move forward, there is an outbreak of paranoia from some of the health unions and some elected officials telling us to remember to continue to quake in our proverbial boots. ‘Global pandemic,’ ‘PCR tests’ and whatnot. Hearteningly, the policymakers and Government leaders have been taking a sober, balanced cost/benefit approach, increasingly focusing on a twin inescapable set of priorities: ‘Lives AND Livelihoods.’ One without the other is a chimera, a pure illusion.
Whether we like it or not, we have only to look at Fitch’s recent action re the downgrade, the protests as daily wage earners despite Government assistance simply cannot subsist or survive. We have import restriction inputs needing review – a message forcefully though supportively delivered from key economic trading partners (the EU recently). There is tourism to enable and to restore, industries that need time and manoeuvring space to stabilise and rebound. All this needs a strategy whereby we can stay the course, keep our ‘COVID antennae up’, but shift more to rapid Antigen testing and not the distortions of mass PCR testing (more and more of the world is coming around to this – Europe is awash in lawsuits relative to what is being asserted to be a clearly flawed testing regime).
And we must stop conflating ‘positive tests’ with ‘cases.’ Only the latter should trigger heightened emergency action. And we need much more rigour in terms of what we classify as a ‘COVID death’ as repeatedly mentioned, in line with insights shared by the Army Commander weeks back.
But we’re not dealing with this in a vacuum, and the sheer ‘presence’ or ‘absence’ of ‘positive tests’ or the mildest uptick in mortality (with very dubious protocols of ascribing such deaths), cannot overtake all other medical considerations, overwhelming concerns re economic solvency, people’s civil rights and right to be with family and loved ones. No one ‘voted’ or ‘agreed’ to have this serious but far from unique viral challenge mutate into an existential scarecrow and overtake all other facets of life and livelihood, to become the linchpin of all that matters.
Why is it prioritised over all else, including things clearly far more lethal? And we must stop behaving as if that is ‘self-evident.’ On the facts, on the global facts, put it to business leaders and people at all levels, and let’s see if they wish to cower over something that admittedly will be around for some time, and which a vaccine may never fully eliminate.
Offer the choice. So, either let’s stay careful and carry on living lives, or destroy everything else about our lives, amplify poverty, destroy education, devastate our economic competitiveness? Not sure how this is still even an open question?
Some less than clear facts
COVID ‘deaths’ are scandalously assessed in too many jurisdictions.
As an example, in two New Jersey hospitals recently, in a sample of 1,380 admissions with COVID-19, of the 640 who died from it, 570 (or 89%) had DNR (‘do not resuscitate’) orders PRIOR to admission, nothing to do with the progress of COVID. In other words, roughly 90% of these ‘COVID deaths’ were already deathly sick, on the literal precipice, before getting the disease, much less dying!
Johns Hopkins after being assaulted by the keepers of orthodoxy, withdrew a paper by a researcher who dared point out there were essentially ‘no excess deaths’ from COVID in the US this year. When we see 260,000+ being cited, it is easy to call her a kook or a quack. However, her point was that if ‘from COVID’, these additional deaths would be concentrated in the 60+ age group with comorbidities where the COVID deaths continue to be overwhelmingly pegged by the US CDC and virtually all global assessments (we often have fluctuating death rates with a band of 10-15% over a five-year spread of years, and if this holds, through year’s end, it would represent +13% in raw aggregate numbers, without commenting on whether they were all actually ‘from’ COVID).
But these numbers showed an ‘equivalent’ rise in deaths at all age groups! Hence this researcher said they were a) either labelled incorrectly or b) COVID was not the primary cause of death or c) as being seen worldwide, many of these were caused by ‘lockdown’ (deferred care, suicides, overdoses or otherwise).
At any rate, the rush to pull the paper has overtaken any proper analysis of this. But hardly, at 13% or likely less, a killer plague. In fact, the 13% excess deaths expected, would be 300,000 as cited by CDC. Even there, they only ascribe 66% of that to COVID. That means, even taking government numbers literally there, COVID ‘may’ have added 6.5% to annual mortality in the US, the worst hit COVID epicentre in the world. But then, curiously, after week 20, CDC stopped keeping track of influenza numbers (evident by visiting their website) …so speculations continue.
Coming to Europe
Autumn arrived; ‘positive tests’ disguised as ‘cases’ dutifully swelled. Daily deaths, rose in line with this, in fact they were seemingly ‘higher’ than Spring levels, allowing for orgies of recriminatory panic and fear, and of course the repeatedly ‘discredited’ modellers flew into the fray, promising 4,000 deaths a day.
However, all-cause mortality however did not budge, which makes a bit of a fudge of the above surely?
So, essentially, there is a major problem with PCR testing, and it is creating the optical illusion of a pandemic that is simply not supported by the mortality numbers or other facts.
The UK summary by leading researchers:
Essentially, if we can replace PCR tests, here in Lanka, and elsewhere, by and large with Antigen tests, or Lateral Flow Tests, and keep PCR for reinforcement or rechecking only where we have the presence of symptoms and the Antigen tests are testing negative, we will resolve much of this hysteria in one fell swoop. In Liverpool, almost 90% of the ‘cases’ disappeared when re-testing was done, particularly among the asymptomatic needless to say. (Once more, PCR tests are highly sensitive, and can pick up ‘fragments’ or ‘debris’ and do not testify to the presence of ‘live’ virus.)
Defining an epidemic
An ‘epidemic’ is a mass spread of an infectious ‘disease.’ COVID-19 is the actual disease, and this requires definitionally ‘symptoms.’ Somehow, though WHO first said there was no asymptomatic spread, they then backpedalled under pressure but still said it was ‘extremely rare’ and that most of the spread happened via symptomatic individuals. Other experts are far less timid in questioning the ‘viral load’ of someone ‘asymptomatic,’ though that should be kept distinct from ‘presymptomatic’ (where there the viral load is building, and there is clear contagiousness).
Contrary to those cautions, we are now in massive derangement chasing down the healthy, immune population, and over-testing madly. If influenza was tested for in the same way, with such porous parameters, we would have been locked down each winter for a millennium.
The very definition, in medical literature, of a ‘false positive pseudo-epidemic’ is an exponential rise in diagnosed cases but no excess deaths. We were on the cusp of this with Swine Flu in 2009, essentially stopped by halting PCR testing then and switching to antigen testing.
UK death classification is also dicey, with anyone testing positive in a 28-day period, even incidentally, being labelled a ‘COVID death.’ That this is causing distortion is further verified by the lack of rise of pneumonia on death certificates this time around, which was very clear in Spring. In fact, shockingly, Accident and Emergency attendances for acute respiratory infections are roughly as Clare Craig, a leading UK pathologist pointed out, currently about 300 per day lower than average.
As per the former Chief Science Officer of Pfizer, Michael Yeadon, writing with other medical and scientific colleagues, “The PCR-based system routinely reports positivity values exceeding the absurd, and these are accepted without comment. This has been allowed to happen because the assumption is that PCR is high science and cannot be far wrong. Nothing could be further from the truth.”
Some clear guidelines emerge therefore
We should stop mass testing asymptomatic individuals. If still in doubt, five days of home quarantine, just in case. But since we are not in an epidemic in Sri Lanka by any definition of exponential growth of real ‘cases’ or ‘clear deaths’, mass testing has to be carefully justified.
PCR testing should revert to the original stringency that was required at the outset, ‘all three genes to be positive,’ not just one as we have lapsed into today. While that may read as esoteric, all the medical and scientific professionals will understand that this was clearly applied in Spring.
Any future ‘outbreak’ must be Antigen test assessed and aligned with symptoms over a few day period, and where necessary, with confirmatory PCR testing but in well-managed laboratories, when and if symptoms and evidence of direct contact seem to clash with Antigen (which is 85-90% accurate during the period of peak contagiousness) findings.
Let’s understand the simple math outlined previously re ‘false positives.’ Say 1% of the population has the disease. This is pretty standard, so if true here, it would be 210,000 are infected (would be considered very low prevalence, not basis for a panic). Assume the test used has a mere 1% false positive rate, correctly picks up 80% of true cases (so 20% false negative rate).
Now, on these assumptions, take 1,000 people, 10 false positives would emerge +8 out of 10 test positive (10 actually have the disease). So, you would get 18 positives, of which only 8 are ‘correct’ namely 44%. Over half the positives would therefore be false in this extremely likely scenario!
That we have gone this long without a public operational FPR (false positive rate) for COVID is beyond absurd. And without answering what that is, you should not listen for 30 seconds to the next ‘specialist’ or ‘politician’ intoning about ‘danger’ in sepulchral tones, looking dutifully ominous, while they enjoy their moment in the sun. First tell us FPR, then let’s talk. It is sheer negligence to perform what is anyway not really intended as a ‘diagnostic’ test for ‘diagnostic’ purposes without even knowing what the results mean!
And one further spanner in the works. WHO said weeks back that its best estimate was 10% of the world’s population had already been infected. If so, that’s 750 million people, and therefore then a global Infection Fatality Rate (IFR) of .14% only. If Lanka has had 10% of the population infected, that would be 2.1 million people! If 116 people say are dead from that (just granting that for purposes of analysis, despite all the caveats before), then our IFR would actually be .0052% rather than .45% or .5% (still extremely low by global standards, and distorted by what we are calling ‘COVID deaths’ as explained), and that certainly does not mandate further economic and social self-destruction.
Maskerade
Masking is less of an issue, but it is one, as I cannot imagine to what numbers things would have to fall, for us to move past this. It is quite curious, back in February and March, health experts were opposed to masking. On 29 February, the Surgeon General of the United States said, “Seriously people – stop buying masks. They are not effective in preventing the general public from catching #Coronavirus…”
Our fickle Fauci, Director of the National Institute of Allergy and Infectious Diseases said, “There is no reason to be walking around with a mask.”
WHO warned against masks, “WHO stands by its recommendation to not wear masks if you are not sick or not caring for someone who is sick.” (30 March)
Early April, New England Journal of Medicine wrote: “We know that wearing a mask outside health care facilities offers little, if any, protection from infection…In many cases, the desire for widespread masking is a reflexive reaction to anxiety over the pandemic.”
And then, the tide turned, though no new scientific basis has been asserted, no new trial is pointed to, no fresh ‘finding’, nothing. We are to believe that somehow the ‘symbolism’ of the pandemic overtook us? That selfsame Surgeon General now said, “You wear your mask to protect me…I wear my mask to protect you.”
By June, the New England Journal claimed they were misunderstood! But the direct quote is above! They were campaigning for ‘Orwellian distortion of the year’ award by this stage. Journalists, in possession of their senses, should have challenged the unsubstantiated about turn, but instead took on the new evangel as an arbiter of social responsibility.
Both in the US, and certainly now in Europe, the most assiduous mask wearing regimes have reported the greatest surges not only in ‘positive test results’ but seemingly in terms (relatively speaking) of health issues and real hospitalisations. Any other time in history we would have said this ‘failed.’ Now we say ‘more mask wearing’ was needed!
Surgeons and transmissibility
Infected people we are told exhale viral particles, carried inside larger molecules called ‘aerosols’ or ‘droplets.’ If those close to an infected person inhale those, they are exposed to the virus. Aerosols are smaller, but a ‘droplet’ is not what it sounds like. It is not a small visible particle say like a ‘mucus ball’ which someone with a cold may sneeze into a handkerchief.
Both of these particles are far too small to be seen unaided, and so any benefit of the masks is at the invisible level, not re visible spit or something akin to that, for which they can be helpful. But the virus mostly travels on much smaller particles.
To catch those tiny aerosols and droplets you need essentially a respirator. The most common model in the US is called an N95. Surgical masks offer much less protection (surgeons tell you their masks are not designed to rebuff viral particles, but personal respiratory droplets) and cloth masks have virtually no standards relative to this at all. Moreover, N95 and other respirators are ‘sealed’ and ‘fit tested.’ So no unfiltered air between edges and skin. Surgical masks are sealed too, and are designed for wear in an oxygen controlled environment, which enriches oxygen supply and keeps the right balance with CO2 (which we exhale, and with many masks, we are just then breathing in our own waste, which virtually any medical source will confirm is far from healthy). Neither are meant to be worn for more than a few hours.
With the everyday masks, besides the very minimal protection, and beyond the gaps between mask and wearer, eyes are exposed too of course. The overall medical consensus stated by Dr. Michael Osterholm, an eminent infectious disease expert, “Standard cloth and surgical masks offer next to no protection against virus sized particles or aerosols. I’d prefer to have people focus on staying three to five feet apart.”
In fact, while closed, tight spaces are the main issue, we have reasons to think viral particles do float in rooms, for a little while. Chinese experts encourage ‘keeping windows open,’ and therefore the silliness of locking people up inside, or being ‘masked’ outdoors, particularly when no one is in their personal space. This is sheer silliness, unhealthy (re oxygen supply), and purely superstition.
A trail of trials
A February Hong Kong review of trials testing masks outside hospital settings relative to the flu found no evidence that masks reduced ‘laboratory confirmed influenza transmission.’ Back in 2015, Vietnam tested re ‘cloth masks’, and found those who wore them were more likely to develop infections! Cloth masks stopped only 3% of particles in the best case, medical masks just over half.
Much maligned though it has been again by the keepers of orthodoxy, on 18 November we finally had publication of a Danish peer reviewed trial covering 5,000 people in the spring. Half wore high quality surgical masks (provided for free), the others no masks; 53 people in the maskless group were infected in one-month time, compared to 42 who wore masks. The totals are nominal enough to be cheer-giving either way. Such a differential they found indistinguishable from chance.
Among those who wore masks they further separated those who wore them ‘always’ or those that exercised ‘choice’ (still possible in Denmark!). Among that subsection of ‘always’ versus ‘maskless,’ counter-intuitively, an even smaller difference! And for all the brickbats hurled against the study, since there isn’t one randomised study in the affirmative, why don’t we invite the self-righteous to do one, and thereby set the record straight?
Now, relative to whether I’m protecting you, this comes down to whether asymptomatic transmission is credible, the size of particles we exhale, and the number of viral particles needed to cause an infection.
We do exhale large droplets of course, which a mask could catch, so they can help in some ‘close’ settings. But a remarkable paper in the medical journal Lancet in September 2020 by Kevin Fennelly, a pulmonologist concluded that consistently pathogens are found in small particles, infitesimal ones, called ‘microns.’ Two thirds of influenza was contained in particles under four microns. Infectiousness also tends to go ‘up’ as size of particles goes ‘down’, as these invisible small particles penetrate more deeply into lungs and other organs. Fennelly has called therefore for ‘air disinfection with ultraviolet germicidal irradiation’ especially for nursing homes and the like.
If you are sick, certainly everyone is urged to stay home or get care, and if you must go out, definitely wear masks, a way to also signal extra care is mandated. However, despite again, initially a chorus of experts, including brother Fauci and even now the WHO troupe saying asymptomatic transmission is rare and is not the way such illnesses spread and more, of course some studies were pulled out that allegedly show people with no symptoms having high levels of the virus.
However, when seeking a translation of that to find actual evidence (via contact tracing) of this phenomenon, no corroboration has been forthcoming! Four studies, as per WHO found only 0% to 2.2% of such transmission cumulatively. In May, in Wuhan researchers tested everyone: 10 million tests conducted; 303 tested positive and were asymptomatic. Upon contact tracing, no infections! Their conclusion: ‘There was no evidence of transmission from asymptomatic positive persons.’ Not definitive perhaps, but definitely instructive.
Here on the homefront
So, Lanka needs a fighting chance to throw off the misleading mantra of Covidian doomsday scenarios.
Our case load is objectively modest, and has flattened, and if we switch to Antigen tests, will likely establish a new, less unnerving equilibrium.
Our deaths are mostly with COVID as ‘bystander,’ sometimes ‘contributor’ and only in a minority of cases, the primary cause. Regardless, the number is mild compared to 12,000 monthly national deaths, clearly no net contribution to excess mortality.
Anyone who says Lanka will be overrun has to either register as a soothsayer or else provide a factual, medical or scientific or even sociological basis beyond making an otherwise empty assertion.
We must continue to revise our protocols so that every ‘positive test’ is not a compulsory hospital sentence removed from family and friends. Let us save hospitals for ‘live cases’ and those needing care. If people’s lives are not completely disrupted and potentially decimated, they are likely to cooperate better and come forth faster if symptomatic.
Lanka’s resilience is a remarkable asset. If we can add to it, the ability to sift the essential from the incidental insofar as data, and then create a vital and vigorous results path, then with our leaders, with our neighbours, with our family and with our colleagues, we’ll make this pandemic period more than wreckage. We’ll use everything present to rebuild. High time we jolted ourselves back awake and became architects for tomorrow’s better possibilities.


