Thursday May 28, 2026
Thursday May 28, 2026
Saturday, 5 June 2021 00:10 - - {{hitsCtrl.values.hits}}

Our leaders can lead us. Re-educate the public. This is not Ebola or Yellow Fever, by a long shot. Let people out for fresh air and Vitamin D. Let the bulk of the population not at risk go back to life and develop natural immunity. Guard the elderly and use the early, preventive treatments for everyone who needs them – Pic by Shehan Gunasekara
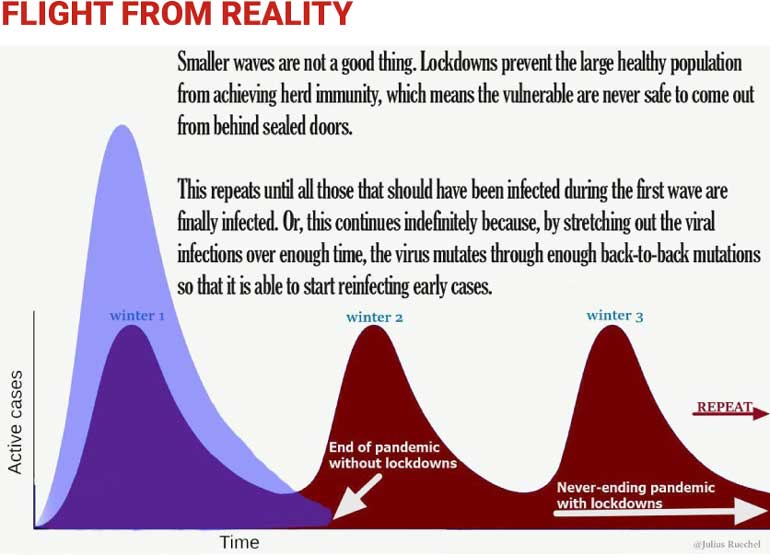
 We are currently throwing a “temper tantrum” against reality, and it cannot end well. The graph pictured encapsulates it and is consistent with all global data and research.
We are currently throwing a “temper tantrum” against reality, and it cannot end well. The graph pictured encapsulates it and is consistent with all global data and research.
The longest-running European lockdown is Germany…coming into seven months! Germany is one of the richest countries in the world and has become a quasi-police state with detention camps set up and closed-down restaurants converted into PCR testing centres. While Sweden, with no mass lockdown, outperforms it in every COVID-related public health measure (including cases and mortality and even economic impact).
The assessment by leading researchers from Munich published in the last few days sums it up: “There is no direct relationship between the reproduction numbers calculated by the Robert-Koch Institute and the enacted measures – neither with the Lockdown Light from 2 November and its escalation from 16 December, not with the further escalation that was enacted at the end of April 2021.”
The UK, having prevaricated for too long, is more open than shut now, and had a vast outpouring of protests, number of COVID deaths on 1 June were zero. Flu and pneumonia have been consistently killing more for weeks.
In the US, by contrast and to the chagrin of the Germans, the Indy 500 race car event, with thronged, packed attendees (about 100,000), only about 5% masked. Florida open since September, 57% reduction in all indicators. Texas plummeting cases over three months now, with 40,000+ in packed stadia and concerts, majority maskless.
So, how do we just ignore this, as if this is some alien reality, and if we just studiously shoot ourselves in the foot, all will be fine? The most protracted lockdown in the world is Peru, which by the way, has the largest number of per capita fatalities, both from COVID and from the disastrous implications of the Lockdown. We surely don’t want to join that group, rather than the flourishing open US States, Sweden, Bulgaria?
Japan never fully locked down, constitutionally barred from doing so. Despite a relative recent “surge,” while having kept society and economy open throughout essentially, they have one of the lowest number of deaths per million in the world. Oh, and just a little more than 1% have been vaccinated.
So, our prescription is to study none of the successes, and for some reason, go madly into perpetuating our economic and social unspooling?
By the way, another study has just emerged, indicating Vitamin D is one of the best preventives, and it is used in early treatment protocols around the world. So again, it seems crazy to be locked “in” given that, once more, there is not one recorded instance of outdoor transmission as I have reported before, reaffirmed by the New York Times and their research a few weeks back as well.
Lanka confusion
Just before the latest infliction of self-destruction was “medically recommended” by a confluence of groups, we were assured there were “medical reasons” to want 14 days, a complete 14-day shutdown. Of course everything was trending down already, and the alleged two weeks were not needed, as “positive tests” were on the decline (we are testing four times what we tested in April, and while positivity has gone up, certainly nothing akin to the optics – from the fickle PCR tests whose Ct settings we cannot get confirmed, nor the number of those “asymptomatic” and therefore not really of interest as these large gatherings all over the UK and US have again proven).
Coming to daily deaths, those actually dying on the day have not exceeded seven to 10 and on most days less (the larger numbers given, “38” or “42” as shown, are aggregates of 10 days, two weeks, or more). Ergo there is no exponential increase. It’s clear we were doing perfectly fine with targeted “shutdowns”, since there is a two week lag in lockdown impact, no one can assert it has saved us. We could manage with far more nuanced “circuit breaking.” Colombo MC has about 140 “positive tests” a day, and so the economic rationale for shutting it down whole-scale seems beyond crazy.
Even how we are filling out death certificates, continues to confound. As per the report, 1 June, one person actually died! The other 42 came from 20 to 31 May, many days just one or two.
Bear with me and actually read indicated summary of causes of death over this period: Chronic liver disease, COVID 19 lung infection, heart disease, atherosclerotic coronary artery disease, pneumonia, diabetes mellitus, acute pulmonary oedema, multi systemic disease, severe COVID pneumonia, acute kidney injury, multi organ failure, septicaemia complicated with C-19, ischemic stroke, hypertension, chronic kidney disease, cancer.
Reading that, is anyone like to bolt inside saying, “unprecedented killer pathogen on the prowl?” No, we will realise many of these good people were going to pass, and in some instances C-19 was a bystander, and in some, it “complicated” or contributed, just as influenza and many other diseases will with weakened immune systems.
Recall, we were just told again it was “medical advice” that we needed suddenly, and inexplicably, more “locking in.” After having been on the record repeatedly, saying there were medical grounds for two weeks, now that morphing into a “needed’’ three weeks for “wave 3,” is hard to take in. Already rumours are flying of it being extended to the 21st “and beyond”.
We’ve already had to go to Bangladesh for a “currency swap” at a high interest rate, and it makes one wonder, is that developing country not facing the same virus? Of course they are, and they’ve used early treatment which I’ve been writing about to come out of their recent surge, by and large they’ve stayed functional, and their exports are flourishing.
India never had a national lockdown, Delhi shut down for some time, but was still functioning in key pockets, and that was in response to the world’s most catastrophic case count in the hundreds of thousands daily. Not comparable. Pakistan, applied brakes over Eid, but is back to functioning, and C-19 numbers are back to where they’ve been with this now “endemic” pandemic, in fact sputtering somewhat. And here we are, frozen in place, somehow “magically” expecting to pull out of the nosedive. But if everything is shut, our businesses cannot compete or operate, how will we possibly do so? This is why being told how to run a society from doctors, is ill advised. Particularly, if they will not deign to update and upgrade their playbook.
Malaysia has just entered a two-week lockdown, reluctantly, having said they have avoided doing so to safeguard livelihood along with lives, as they realise the two are inextricably linked. But then, their numbers are far more alarming. With 31 million people, they have been averaging 8,000 “positive tests” a day, for an extended period, hence they have decided on the “circuit breaker.” And while research indicates it is likely misguided, it’s understandable. Their per day deaths are around 126, an order of magnitude difference as well. Nevertheless, their “lockdown” in relative terms is far saner in terms of health and well-being than ours, and we can hardly allege they are operating outside “medical advice.”
Specifically:
“No more than two people will be allowed to leave a household, and only for specified activities like buying food and medicine or going to work for those with jobs deemed essential.” (Two people makes sense, to carry things, to help each other if both are elderly, or just to minimise people taking excessive time in an establishment)
“No one will be allowed to travel farther than six miles from home except to receive medical services.” (Nice and clear)
“Public transport will operate at half capacity.” (Some provision for those who need to move about, and even in the now dated playbook, ample distancing)
“Stores that are allowed to operate will be open for limited hours.” (So, some shops can be open, over known hours, not a complete paralysis)
“Individual exercise and jogging will be allowed outdoors, but social distancing of at least six feet will be required.” (Far too far, outdoor no transmissibility, but at least they are outdoors, getting vitamin D, staying physically and mentally healthy)
“In an attempt to limit economic harm from the lockdown, key factories will be allowed to operate at 60% of capacity, including those producing food, medical components, electronics and textiles for use in protective equipment.”
There are ways to manage. If against the grain of recent research, we at least assert it’s only two weeks, then let’s stick to it. But, during that period, then let people still live! We need at this stage, more than draconian dictums and garish news items about “arresting the flouters.”
We need the humanity and compassion and empathy for everyday life and viability, that we know our leaders are dedicated to, but have to better express through their policies. More data, less alarmism, more balance, less tunnel vision. There are more things in heaven and earth that deserve leadership and attention than this fading pathogen. Other sources of harm, and alarm and suffering and need are not less important than this over-hyped virus.
From the top once more
It’s not “novel”, coronaviruses have been circulating forever. In the US, C-19 is now already only the fourth most prevalent. If as we are hearing, engineered in a Wuhan lab, was tampered with, but not unique. We know this from antibody resistance, and also T cell cross immunity from those never infected, people exposed to other coronaviruses or colds. Amply documented.
Lethality (also up on WHO website), based on seroprevalence studies from around the world, from the world’s foremost expert on meta-analysis, John Ioannidis of Stanford, 0.15%. Far less deadly for children than flu, about the same for those 20-50, moderately more lethal with pre-existing conditions 50-65, considerably more as you age, and lethal above 80. Global median age of death is 82, particularly if you sift for those deaths where COVID-19 was the primary causal factor. These are not world altering statistics. This tracks normal mortality The Spanish Flu of 1918, which was epochal, by comparison had one-third of the then planetary population infected, and 10% of those died! And it primarily targeted the younger. We cannot even get our heads around equivalent figures today.
As much as 50% of global deaths came from nursing homes, almost 99% of the transmission indoors even once partially open, so “locking in” is a disaster. In Europe no excess mortality in 2020, Asia and Africa none, slightly lower than usual. The UK for example, through the NHS, indicates every year 2009 and back, age and population adjusted for mortality, was more lethal than 2020.
The US once again, age and population adjusted, takes us back to 2003, not the 13th century. Globally, 2017 with a devastating influenza wave, was more lethal globally, adjusting for age and population than 2020! Shocking, all verifiable. Much of the planet (Africa, parts of Asia, parts of South America, Sweden, Norway, Finland, more and more US States), did not stay locked down, or even “masked”, so we know that this is containable and not exponentially of concern.
It’s airborne, and so large droplets are not the issue, hence literal “distancing” is overdone, and we need to create natural immunity. All the recent studies reconfirm what thousands of years of evolutionary history has already demonstrated, immunity lasts for years, likely forever, and it’s not just demonstrated via antibodies, but T Cell coding, which even 17 years after the original SARS, shows clear immune responses from those who were infected then.
By “locking in” we generate more variants, and simply make the pandemic perpetual and cyclical, rather than endemic and manageable.
There is no demonstrated “asymptomatic transmission”, hence all these overflowing stadia and public events, and protests, with no spikes and Wuhan at New Year’s with no sustained outbreak whatsoever. So, if we treat asymptomatic at home, to the extent we treat them at all, and realise these could be false positives from a test that magnifies viral strands and does not testify to live infectiousness, then we can focus on the “symptomatic” and then all of this can be dealt with without panic by our public health professionals.
Beyond this, there are treatments galore. From monoclonal antibodies, now being even FDA approved for all age groups, and a new drug landing in the UAE premised on this, to numerous cheap, reliable, easily available protocols including HCQ (which was slandered by a later retracted and fraudulent paper whose principal is the subject of three malpractice lawsuits; the recent trove of Fauci emails also shows he acknowledges its utility and kept some for his family while misleading the rest of us), Ivermectin which turned India around (and now Mexico has testified to a similar outcome – better mortality stats than the US, with one fourth of the vaccination!), and others.
The trick is “early treatment” as soon as there are symptoms. That is what we do for every other disease or illness. If you find a lump, you don’t say, wait for cancer to invade your cells, and when you’re hospitalised, we’ll do “something.” When early treatment is practiced, we find even 90% of the minority that get infected don’t require hospitalisation, don’t need oxygen or extreme life-saving measures. I have provided links in past articles to resources and will get more of these communicated. Bangladesh used some of these as well to stem the tide, the results are evident.
Dr. Peter McCullough, author of both of the only peer reviewed articles on treatment globally, reminds us this disease has a viral component early, then an inflammatory dimension, and then thrombosis. Each of these elements can be treated, doctors have been doing so for ages, and not treating people early he says, amounts to “therapeutic nihilism” and downright malpractice. To read about attempts to suppress some of these treatments, please visit www.covidcandy.net for a referenced, fact based, shocking expose.
Children virtually never die from this, shrug off the infection, then are immune. They are not vectors of transmission. Jurisdictions like Sweden, Switzerland and Florida have proven that conclusively. Sweden kept schools open throughout, not one death. Ergo, this is an assault on children’s education, we are retarding their social development, we are stifling their emotional health, and we cannot even quantify or catalogue the ongoing ramifications.
The “vaccines” cannot be the solution. The key ones are experimental gene therapy. Not one of them has been authorised anywhere except for “emergency use,” hence the push to suppress natural, cheap, readily available alternatives. None of the trials included the vulnerable or elderly, so we don’t know. They are touted to “suppress symptoms” and we have growing, worrying reports of reinfection, hence life-long booster shots if you go this invasive route.
Adverse effects from all the vaccines, while a small percentage (currently) of those vaccinated mercifully, are over 4,000 deaths in the US (more than 9/11), over 10,000 in Europe, and we are told usually less than 10% of adverse effects get reported. Add them all up, and these are more adverse effects than recorded from all other vaccines combined for four decades if not longer. Ergo, if vulnerable, and elderly, they may be worth it. But early treatment, plus age stratified risk, and natural immunity (demonstrated since the dawn of time, hence we’re alive), is less risky, more enduring, and does not require constant “booster shots.”
So, take these if you wish, and in percentage terms, you’ll likely be fine. But this may not provide immunity even then, and not fortifying ourselves with everything else we’ve learned, is crazy. And on children, beyond clotting, the heart issues and more, realising safety trials won’t be completed until 2023, we are all of us, going through “human trials”. Let’s beware subjecting our children to this, without a very careful review of the real risk data globally, and not from a propagandist website or even local dispenser of these.
There is a reason the Nuremberg standard is called “informed consent.” If you wish to hear more, Dr. McCullough is here in dialogue with an eminent, once pro-vaccine doctor, who radically changed this mind based on the evidence he’s personally seen: https://www.ourfreedomtube.com/v/djSWEv.
In a nutshell then
We are playing with fire, disrupting lives and livelihoods and social contracts, the credibility of Government announcements, with no expressed strategy and confounding “medicine” with “governance.” We have to call time-out and do our own “reset.”
Three weeks here, another variant? We are told by the former Chief Science Officer of Pfizer, Dr. Michael Yeadon, “variants” are at most 0.3% different from the original, and there is no way our immune system if allowed to express itself, is at risk. We can prove this by the English variant being the most dominant in the US where numbers have collapsed, and the so called “Indian” having fizzled out in the UK.
So, another spike, another three weeks? This is a far greater threat to solvency and thereby sovereignty than having to negotiate with the IMF or other strategies or tactics we may have to outgrow our aversion for.
Regardless, our leaders can lead us. Re-educate the public. This is not Ebola or Yellow Fever, by a long shot. Behaviourally our citizens seem to know that, when let out, and the way support was flowing for local businesses and tourism was heartening. So, forget asymptomatic, there are early treatments they can take at home, a globally benchmarked protocol has been published and can be readily referenced. Let people out for fresh air and Vitamin D. Let the bulk of the population not at risk go back to life and develop natural immunity. Guard the elderly and use the early, preventive treatments for everyone who needs them.
Life is not “non-death.” Pretty soon, we’ll be “alive” perhaps but unsure what that means, or what’s possible, and wondering how we lost and waylaid all that makes life worth living.