Thursday Jul 02, 2026
Thursday Jul 02, 2026
Monday, 12 October 2020 00:15 - - {{hitsCtrl.values.hits}}
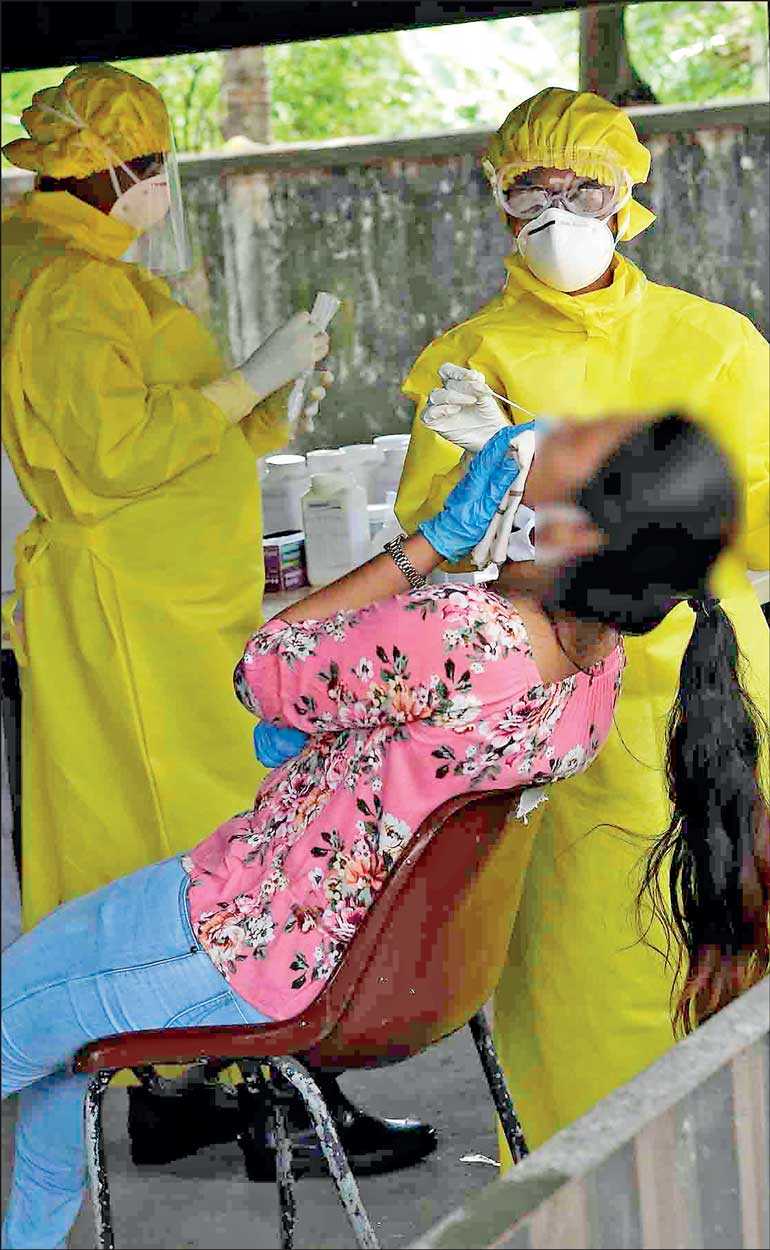
We must wean ourselves off the fascination with the PCR swab test, with a “case-demic” from a fatally flawed (for this purpose) methodology which terrorises people unnecessarily – Pic by Shehan Gunasekara
Sri Lanka, seeking to find its footing once more, enjoying a fragile recovery, is again potentially undermined by an outbreak of cases of COVID. And while policy makers have kept most responses  targeted and focused and local, and this is highly laudable, various ‘manacles’ are going on, psychologically and emotionally and even practically that seem to have taken the wind out of the sails of quite a few initiatives, activities and interactions.
targeted and focused and local, and this is highly laudable, various ‘manacles’ are going on, psychologically and emotionally and even practically that seem to have taken the wind out of the sails of quite a few initiatives, activities and interactions.
After a seeming two months of no local cases, to “suddenly” see a new cluster for which we have no ready answer, and “spot” cases here and there, though in truly negligible numbers, the issue is the official narrative has to be updated, edited, or revitalised to cope with this data.
Undone by tests
As highlighted in my last piece, the PCR test was never intended to be diagnostic. And yet we have an entire planet held hostage by its vagaries.
That it was never intended for diagnosis per se, rather than reinforcing a diagnosis, assuming there was some external “gold standard” (pregnancy for example for a pregnancy test) against which to compare it (there isn’t here, as the test is part of what “verifies” COVID-19 and so what “verifies” that can be asked as the “symptoms” are shared by numerous diseases).
However, beyond that, is the very nature of the test itself. The founder, a Nobel laureate in Chemistry, Kary Mullis, passed away (not from COVID I hasten to add) last year. He clarifies that PCR tests can’t really be “mis-used” but can be “misunderstood.”
Quoting him directly: “I don’t think you can misuse PCR. It is the results; the interpretation of it. If they can find the virus in you at all – and with PCR, if you do it well, you can find almost anything in anybody.”
Well, that is a chilling assessment in light of today’s realities. So, while it is true he had nothing specific to say about PCR tests and COVID (he died before it came to light, which therefore we can stop citing as relevant), his views clearly encompass the current predicament.
Quoting once more: “It starts making you believe in the sort of Buddhist notion that everything is contained in everything else. If you can amplify one single molecule up to something you can really measure, which PCR can do, then there are just very few molecules you don’t have at least one single one of in your body.”
Another specialist has said, this time relative to COVID, that if you have the amplification cycles very low, no one has it. Increase them, then you start getting false negatives, then false positives start popping, and at a high enough amplification cycle, everyone will test positive (above 45 and around 60 say).
Making the ‘case’
Testing ‘positive’ is not a ‘case’ in medical terms, evidence of live infection and needing care for symptoms are defining characteristics. So, we are perhaps misleadingly calling all these “positives” “cases” and saying there is an outbreak of COVID “cases” in, for example, Sri Lanka.
Yet there aren’t as best we know any surges of admission into hospital rooms or ICUs or related mortality spikes. So, all we can say is there was a surge of “positive test results”. 
Imposing police states (as have happened in Victoria, Australia) or egregious never-ending lockdowns (as seen in Argentina) based on these, probably IS “misuse.” A PCR test, says Mullis, magnifies what inferentially seems to be there, but isn’t as clear by far he says, “as the measurement for apples” for example.
By making the “invisible” into something “measurable” it enables study and discourse, though perhaps not conclusive prescriptions, particularly those that destabilise lives and societies.
Tackling the issue of calling everything a “case” Mullis clarifies once more: “PCR is just a process that allows you to make a whole lot of something out of something. It doesn’t tell you that you are sick, or that the thing you ended up with was going to hurt you or anything like that.”
We are amplifying “results” many times over and need to locate the right “amplitude” (according to Harvard, that should be 30, according to other specialists 35; above 37 we get into trouble we are told).
And globally, as Professor Carl Heneghan of Oxford University indicates, a “case” of COVID has no unified meaning and has different thresholds and standards depending on whether you go to WHO, the US, EU, China, Italy, Spain and France.
A quick litany of what we got wrong
Dr. Stadler, a Swiss Molecular Biologist, former Director of the Institute of Immunology at the University of Bern, rails against everything we got confused. To wit:
The virus is not “novel.” Secondly, it was silly to think given similarity of coronaviruses that there wouldn’t already be some immunity present in the population. Third, it was “the crowning of stupidity” he writes to claim “someone could have COVID-19 without any symptoms at all or even to pass the disease along without showing any symptoms whatsoever.”
He suggests young and healthy people walking outdoors with masks would be better placed in helmets as there is a greater risk of something falling on their head, than getting a serious case of COVID-19 under those circumstances.
So, here in Lanka?
Here are the key takeaways that must inform our national decision making.
We have a contagion, which has a global infection fatality rate of .03% on published figures, or if you take WHO’s numbers of 750 million having been infected (10|% of the population), then the fatality rate is .13%, which is the seasonal flu.
Yet our responses have led to small and large business failures, flaring of poverty, interruption to social ties, severing of critical personal contacts in countries…and none of this is what we should want for Sri Lanka due to the potentially unreliable PCR test “positives” as per the above.
There has also been a catastrophic decline of routine screening of diseases, which if detected early, are far more amenable to positive outcomes (like cancer screenings).
Children and young adults, at virtually no statistical risk, are again, here as well as elsewhere, being deprived of educational and development opportunities that simply may not be available again. They cannot keep being “postponed” indefinitely because we are terrified by PCR test hobgoblins (particularly here in Lanka, a country with virtually no COVID deaths even when clusters have flared).
The grotesque mass impact on lives and livelihoods, the infliction of suffering on fellow citizens, we  have to ask how we are measuring or assessing if it’s remotely worth it? The irony is ghastly…telling people to stay home, so potentially ill people infect the healthy, inside, which is the worst environment for eliminating viruses – none of this really helps in preventing transmission of respiratory viruses medical experts keep pointing out.
have to ask how we are measuring or assessing if it’s remotely worth it? The irony is ghastly…telling people to stay home, so potentially ill people infect the healthy, inside, which is the worst environment for eliminating viruses – none of this really helps in preventing transmission of respiratory viruses medical experts keep pointing out.
Globally seasonal viral illnesses are on the rise. Elderly relatives are at risk each year from family members contracting these, and so the same prudence and care needs to be practiced.
Median age of those who sadly succumb to C-19 is over 80, so the above comparison is apt. Lethality is far lower than feared, as again outlined above. More people have immunity, including T-cell and not just antibody immunity, than forecasted. So more exposed, and more with immunity from exposure to other coronaviruses most likely.
We must beware of sounding the crisis horn unduly. If indeed COVID flattens out to be akin to seasonal influenza which experts around the globe are now indicating (and which data other than perhaps in parts of the US, Brazil and India would reconfirm and fortify), so with roughly 1 death per 1,000 infections, then we have to wonder by comparison what would happen if we kept flashing “car deaths” every hour on the hour, or those from cancer or hypertension, or even the 1.6 million TB deaths globally and that’s with a vaccine!
From an actuarial perspective, this is therefore not a leading cause of death globally, certainly not there now with 60 million annual deaths from various causes.
The key question
So, why are we retarding our recovery engaged in an extreme battle to prevent the spread of a single, as it turns not very remarkable respiratory virus (as attested to by leading epidemiologists in Oxford, Cambridge, Stanford, Yale, Harvard, Johns Hopkins…), using methods that don’t work, while being willing to pay a price for this folly which is the indirect and largely avoidable pain and suffering to millions, literally millions of those around the world (from medical impact, to poverty, to educational impact, to mass collapse of businesses and ways of life…)? Have we ever debated the sanity of this so called “lethal calculus?”
And whatever mistakes were made in the early fog of pandemic panic, we surely now know better…how to protect, how to treat, the scale of the challenge, how only very rarely to ventilate (not a disease as leading front line doctors have told us of airway obstruction, but impaired gas exchange needing oxygen masks). We are more alert to clotting disorders and have a trove of anti-coagulants at the ready.
We perhaps know that “suicide until vaccine” is more “homicide by myopia” as it won’t be a panacea, vaccines are simply not very effective for the old and highly unwell. A well-functioning immune system is a usual prerequisite for a vaccine to help it rally.
Seeking a “techno fix” to an “adaptive challenge” which requires paradigm expansion, trusting to the immune systems we were gifted with, intelligent prudence, medical guidance, shared discipline, all coming together, is foolish.
Awaiting a vaccine for an “infection” most people overwhelmingly do not fall ill due to, and most of those who are made ill do not require hospitalisation as a result of, seems strange, extreme, and if you’ll pardon the pun, “fevered.” It doesn’t mean we won’t offer the vaccine, but the nature of this beast does not lend itself to triumphantly finding “the antidote!”
As for “long COVID”, yes let’s be vigilant, but again it’s not a new phenomenon, you get a certain percentage of prolonged consequences for people from flu and influenza too. No signs yet that “long” happens more frequently with C-19 compared to flu, so “proactive hyperventilation” to feed the slightly sputtering panic meter is really not merited.
Relative to “immunity,” viruses mutate, so we are “more” immunised rarely “completely” immunised, and subsequent strains tend to be milder and less lethal as per epidemiological trends over time.
Since nine months or so of data definitely favours the acquisition of immunity from surviving the virus (which 99.94% do), add to it prior immunity, add to it 5% of the population which are younger children who are demonstrably only at nominal risk and do not meaningfully contribute to transmission, and then add the fraction infected and now largely immune, and we are hovering close to this enticing “herd immunity” already most likely.
That does not mean, let me reiterate, that no can test positive, or even that no one can “catch” this or die from what is a serious virus. It does mean there are too few people to support a large and growing outbreak across the country.
Back to the testing
Usurping liberties is not the solution. Further inflicting damage to our economy is not the solution. Trying to “order” a virus around is not the solution.
And we must wean ourselves off the fascination with the PCR swab test, with a “case-demic” from a fatally flawed (for this purpose) methodology which terrorises people unnecessarily.
Sri Lanka needs to safeguard its wonderfully privileged immunological status to date, leverage the concerted leadership and dedication of public servants and front-line doctors and nurses. And we also have citizens aplenty who need a chance to match their enterprise and energy with the courage and heroism we’ve seen and help us economically and socially get past this scourge.
Let us therefore “test” our resolve, our prudence, our wisdom, and our capacity to sift the essential from the incidental, as we decide to move decisively past a potentially misleading or certainly inconclusive testing regime, trust to immune systems and our medical expertise here, and allow ourselves to move into an ever more robust recovery.


