Monday Feb 16, 2026
Monday Feb 16, 2026
Monday, 11 July 2016 00:00 - - {{hitsCtrl.values.hits}}
 By Dr. Amara Satharasinghe, Director General, Department of Census and Statistics
By Dr. Amara Satharasinghe, Director General, Department of Census and Statistics
The elderly population in Sri Lanka has grown rapidly in the past several decades. They were an unprecedented 2.5 million in 2012, and this is still increasing. One in eight Sri Lankans is 60 years or over. This is in contrast to about a sparse one in twenty persons a few decades ago. Demographers project that the aged will double by 2041. Every fourth person in the country will then be elderly. The numerical growth of the elderly has been happening almost invisibly and inaudibly, Can we turn this hitherto helpless and dependent population into a valuable resource and a people that enjoys the evening of their precious lives. It is time to pay a concerted attention to this question.
Most countries of the developed world have accepted the chronological age of 65 years as a definition of ‘elderly’ or older persons. While this definition is somewhat arbitrary, it is many times associated with the age at which one can begin to receive pension benefits. At the moment, there is no United Nations standard numerical criterion, but the UN agreed cutoff is 60+ years to refer to the older population. Lacking an accepted and acceptable definition, in many instances the age at which a person became eligible for statutory and occupational retirement pensions has become the default definition. In Sri Lanka too, cutoff 60 years and above is used to refer to the older population. The elderly are grouped into two categories: the ‘young old’ i.e. aged 60-79 years and the ‘old old’ i.e. aged 80 years and above.
 Demographic transitions
Demographic transitions
Demographic transition is a model used to represent the transition from high birth and death rates to low birth and death rates as a country develops from a pre-industrial to an industrialised economic system. While Sri Lanka was still a developing country, the population experienced a demographic transition. The age structure of the population in Sri Lanka has changed considerably over the past three decades. Decreasing child population and increasing aged population are the striking changes. For example, the child population (below 15 years) has decreased from 35.2% in 1981 to 25.2% in 2012, while the elderly population (above 60 years) has increased by 6.6% in 1981 to 12.4% in 2012. The percentage of people in the working age (15 – 59 years) has also increased from 58.2% 1981 to 62.4% in 2012. These changes in dependent population and an increasing working age population is a demographic dividend or a great opportunity to be wisely utilised for social and economic development.
Sri Lanka has experienced a growing trend in population aged over 60 years since the 1950s, as a result of declining mortality and fertility rates. Starting mid 1940s the death rate declined from 19.6% to 6.0%. Subsequently, the fertility rate or the average number of children born to a woman also began a downward trend declining from 5.5 to 2.4. This trend was accompanied by a fall in birth rate from 37.4% in 1946 to 7.5% in 2012. Consequently, the life expectancy at birth increased steadily. An average woman in Sri Lanka can expect to live 77.2 years, and an average man 78.6 years.
Window of opportunity
This age structure transition in Sri Lanka has produced a demographic dividend, which is conducive for an economic takeoff. In this transition, the proportion of the working age population, aged 15 - 59 years (strong and young work force), is significantly larger than the proportion of the dependents. This is called a “window of opportunity” or a “demographic bonus”. According to demographers, this dividend will not last long since the elderly dependency is increasing rapidly. Therefore, this is an opportunity that needs to be used immediately.
Healthy lifestyles
The changing age structure has many and serious implications in almost all aspects of life. The disease profile has already changed from a predominance of infectious and acute disease to rising chronic, degenerative, and expensive to treat diseases. The ageing population will increasingly put pressure on health systems with the rise of chronic cancer, diabetes and cardiovascular diseases etc;. Older people have a need for more health monitoring and treatment than younger people and the pattern and causes of their illness are different. They need extraordinary care and geriatric treatments that are expensive. Therefore, the provision of long term health care is a most serious issue. Promoting healthy lifestyles and broadening the use of clinical preventative services are critical to preserving the health of older adults and reducing healthcare costs and long-term care needs.
Health in 2014
To meet the demand for much needed data on disease prevalence, at the request of and in collaboration with the Faculty of Community Medicine of the University of Colombo, the Department of Census and Statistics conducted a year-long household survey on health in 2014 covering the whole country. The survey assessed the prevalence of chronic and acute illnesses, accidents, regular use of alcohol and tobacco, etc. This probably is the first countrywide survey of self-reported (without medical tests or clinical examination) health status in Sri Lanka. Self reported health surveys have been demonstrated as a valid and appropriate method for estimating many health related parameters. An annual sample of 25,000 housing units was selected to give reliable estimates by district level in the year 2014.
Data collected in this survey include: prevalence of illnesses; chronic and acute; place from which the treatments were received; accidents; place of accident; health screening; smoking and alcohol use; possession of health insurance etc. Some summary findings are given below.
Diabetes, high blood pressure, heart diseases, stroke, cancer, asthma, mental illness, arthritis, and epilepsy were chronic illnesses considered in this survey while acute illnesses covered diarrhoea, vomiting, fever, headache, cough, stomach-ache, wheezing, sore throat, joint aches and skin diseases. The variations of overall disease prevalence and other indicators by sex, age, geographic location, occupation, industry and employment groups are given in the report (“National Survey on Self-reported Health in Sri Lanka 2014”) released to disseminate the findings.
High blood pressure
According to the survey, the most prevailing (27.3%) chronic illness is high blood pressure. This is followed by diabetes (18.0%). Prevalence of arthritis and asthma are 8.0% and 5.9% respectively.
Findings of the survey on elderly population are briefly presented here. Chronic illnesses are those that persist for long time periods.
Chronic illness, as can be expected, increases with age. Almost 55% of elderly population suffers from at least one chronic illness. That is one in two of elderly persons is living with a chronic illness. This is so with both men (55 %) and women (56 %). However, at the lowest levels of education – grade 5 or below – many more women (80%) are suffering from a chronic illness compared to men (37 %).
This is a very wide gap which merits further study and action. In the population as a whole, about one in 5 persons (18 %) is affected by one or another chronic illness.
There is a clear difference in prevalence of chronic illnesses between economically active and economically inactive elderly populations. Among the economically active population, the prevalence among men is 42% which is very much less than prevalence among females (61%). Among the ethnic groups, prevalence of diabetes and high blood pressure is highest among Sri Lankan Moors. Prevalence of diabetes in this group is 29% and 37% respectively. These percentages for total elderly population are 18.0% and 27.3% respectively.
The need for public screening programs
This survey asked respondents whether they ever checked blood pressure, blood glucose and blood cholesterol levels. Among the elderly population 86% has ever checked their blood pressure. Little above 75% has ever checked blood glucose and 58 % has checked cholesterol levels. From the elderly population not reporting high blood pressure, only one fifth has ever tested.
Similarly, among those not reporting diabetes, only one in four has ever tested blood glucose. Only one third of persons not reporting heart disease has ever tested blood cholesterol levels. These findings may have implications on public screening programs for early detection and preventive care.
An acute illness is an illness that onsets very rapidly and is of short duration. Interestingly, acute illness among elderly is not different from the population as a whole.
Approximately 15 % of people have experienced an acute illness over the one month prior to the survey. The elderly population is as could be expected affected much more by chronic than acute illnesses.
The elderly persons are more vulnerable to accidents. About 16 elderly person have experienced an accident compared to 11% in the general population, and half the accidents have happened at home.
Smoking and alcohol among the elderly
Perhaps an unexpected finding is that smoking and alcohol consumption by the elderly is very much higher relative to the whole population: smoking is three times higher (17 %) and regular alcohol consumption is nearly four times higher (16 %).
Further, from the Census of Housing and Population, 2012, it was found that one third of the elderly population is affected by functional disability: disability in vision, hearing, walking, remembering and concentration, self-care or speaking.
Insurance cover among the elderly
Despite very high levels of health problems, the elderly in our country seems to have little recourse to protective measures. For example, insurance coverage among them is very low (3.2%) and which is much less than in the general population (11.3%).
Good health is a major factor in the quality of life. A good quality of life of the elderly is an important aspect of the quality of life of the entire population. The implications of quality of life span wide across many areas of the life of people such as a happy and contended life at individual level, and resource allocation and utilisation for growth and development at macro level.
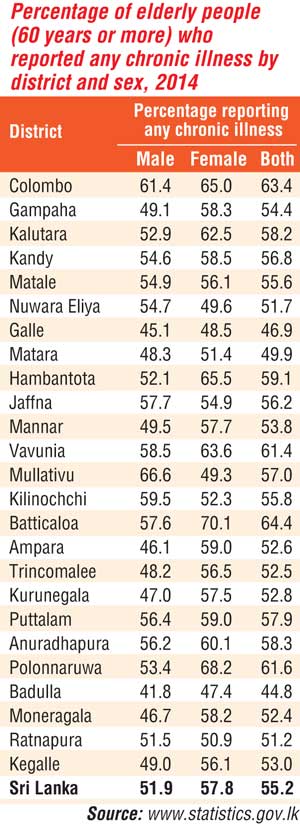
The Table below summarises chronic disease prevalence within districts and brings out the differences between men and women.
The report of the survey with details of findings is published at the website of the Department www.statistics.gov.lk.


